Fig. 7.1
To identify any area of localised tenderness of the lateral chest wall, the patient is rolled on her side in order to let the breast fall away and to examine the site of the pain (left). Equally, to examine the medial chest wall tenderness, the patient is rolled on her side. The breast falls away and it is easier to palpate the costochondral junctions (middle). To examine the lower chest wall tenderness, the breast is lifted upward with one hand, while the other hand presses gently on underlying chest wall to identify the localised pain (right) [1]
Laboratory studies are generally not useful. A pregnancy test, however, should be considered in women of reproductive age if the history or examination suggests pregnancy. Other hormone levels (e.g., oestrogen, progesterone and prolactin) are typically normal in patients with breast pain.
Imaging studies are frequently utilised in the evaluation of the breast. A mammogram should be considered especially in women with a family history of early BC. The risk of malignancy after normal findings on mammographic evaluation for breast pain is about 0.5–2 %, mostly in postmenopausal women. It is unclear whether the pain is related to the cancer or whether this symptom initiates a breast evaluation in which an asymptomatic cancer is identified. Breast pain secondary to malignancy is typically unilateral and persistent. In these cases, imaging with directed ultrasound may be a more valuable assessment tool.
A variety of conditions can result in pain perceived in the breast as a result of pregnancy, mastitis, trauma, thrombophlebitis, macrocysts, benign tumours or cancer; however, only a minority of breast pain is explained by these conditions. Most breast pain is of unknown cause, and the above conditions can be revealed as a result of a directed history and physical examination. As appropriate, an exam directed at the cervical and thoracic spine, chest wall, shoulders and upper extremities, sternum, heart, lungs and abdomen may be helpful in assessing other potential causes of the pain.
CLASSIFICATION. Breast pain is commonly categorised into three classifications: cyclic mastalgia, noncyclic mastalgia and non-mammary pain. Our personal classification scheme is shown in Table 7.1.
Table 7.1
Our personal classification of mastalgia
Classification | Characteristics | Notes |
|---|---|---|
Cyclic mastalgia (about 60–70 % of cases) | Pain varying with menstrual cycle, not to be confused with premenstrual syndrome | Pain charts are an important aid to assessment |
Women without periods, with ovarian function | ||
Pain in the monthly patterns (women without periods or post hysterectomy) | ||
Pain using cyclic hormone replacement therapy | ||
Noncyclic mastalgia (about 20–25 % of cases) | Idiopathic mastalgia | True mastalgia remains a mystery |
Usually a variable and unexplained symptom | ||
Painful breast pathology | Many breast conditions could occasionally result in breast pain; however, only a minority of breast pain is explained by these conditions | |
Stretching of Cooper’s ligaments | ||
Sclerosing adenosis | A highly significant association exists between the severity of mastalgia and the extent of ductal mammary ectasia | |
Mondor disease | ||
Pressure from brassiere | ||
Fat necrosis from trauma | ||
Hidradenitis suppurativa | ||
Focal mastitis | ||
Periductal mastitis | ||
Stretch cyst(s) | ||
BC (rare) | ||
Non-mammary pain (about 10–15 % of cases) | Chest wall pain | Underlying musculoskeletal pathology may be steadily symptomatic or occasionally exacerbated by lifestyle, increasing activities, and ill-fitting brassiere |
Tietze’s syndrome (costochondritis) | ||
Localised lateral chest wall pain | ||
Diffuse lateral chest wall pain | ||
Radicular pain from cervical arthritis | ||
Non-chest wall pain | ||
Gallbladder disease | ||
Ischemic heart disease | ||
Esophagitis and hiatal hernia, especially associated with abuse of alcohol |
Cyclic mastalgia occurs in premenopausal women and is clearly related to the menstrual cycle. The pain is typically bilateral and diffuse, often located in the upper outer quadrants of the breasts with frequent radiation to the axilla and the ipsilateral arm. Occasionally, breast pain may be unilateral or more intense in one breast.
Noncyclic mastalgia may involve continuous or intermittent pain that does not concur with the menstrual cycle. The pain is more often unilateral and localised with the pain in the lower inner portions of the breast. Noncyclic breast pain generally occurs in older postmenopausal women.
Non-mammary pain may present with the symptom of breast pain. Following the history and physical exam, differentiating breast pain and pain radiating from the chest wall or another site is usually straightforward. Occasionally the origin of pain is not evident, or there are multiple origins of pain, making evaluation more challenging.
PAIN CHART. The main form of assessment to confirm the cyclical nature of the symptoms is a breast pain chart, a diary where to document and score pain on a daily basis as either severe, mild or no pain at all. The commencement of menstruation is also recorded, and after a couple of months, it becomes apparent if the symptoms are cyclical in nature.
A breast pain chart can be used to record the pattern and severity of the mastalgia, as well its relation to menstrual period. Many different models of breast pain record chart are available. Our personal chart takes account of three scores of mastalgia (light, medium and severe) according to intensity (assessed using the visual analogue scale) and to duration of the pain (Table 7.2).

7.2 Cyclic Mastalgia
Clinical Practice Points
There are considerable overlaps between cyclical mastalgia and premenstrual syndrome, but there are also significant differences, requiring different approaches.
A pronounced pain characterises cyclic mastalgia so that it should not be confused with premenstrual syndrome, even if cyclic mastalgia and premenstrual syndrome have substantial overlaps.
Cyclic mastalgia includes pain varying with menstrual cycle as well breast pain in women without periods but with ovarian function (i.e. post hysterectomy) or even postmenopausal ones taking HRT.
The basic cause of cyclical mastalgia is clearly endocrine in nature, but the precise mechanism(s) continues to elude investigators.
In cyclic mastalgia, pain charts are an important aid to assessment.
Virtually all women will experience a degree of pain or discomfort in their breasts at some time of their lives. This is normal and most often occurs in the week prior to menstruation. Cyclical mastalgia is not to be confused with premenstrual syndrome (PMS), which, by definition, is associated with the menstrual cycle but differs in presentation, effective treatment and likely aetiology (see Chap. 3). In some women, however, the pain can become quite severe and in certain cases can result in problems with daily activities, quality of life and marital relationships. When this occurs, cyclic mastalgia should be treated.
Due to the relationship with the menstrual cycle or hormone replacement therapy, it is thought that the cause of cyclical mastalgia is hormonal. Actually the aetiology of mastalgia is not well understood. Hormonal assays of oestrogen, progesterone and prolactin have shown no consistent abnormalities despite the relationship to the menstrual cycle. Even so, pregnancy, lactation, menopause, oral contraceptives and hormone replacement therapy variously affect the course of breast pain. Some studies have shown hyperresponsiveness of prolactin to stimulation by thyrotropin-releasing hormone, while others have suggested elevated levels or abnormalities of lipid metabolism. It has been proposed that breast pain during the luteal phase of the menstrual cycle may be due to higher serum oestrogen-to-progesterone ratios. This may be related more to an insufficiency of progesterone rather than an excess of oestrogen.
One correlation between women with mastalgia and controls when determining total body water was not found. Therefore, as fluid retention is not a factor, there is no rationale for the use of diuretics or sodium restriction.
There are also other suggestions that consumption of too much caffeine or a deficient intake of essential fatty acids can also result in cyclical mastalgia. However, no explanation has been demonstrated with evidence, and in many cases cyclic mastalgia still remains a mystery.
Symptoms. Cyclic mastalgia affects up to 40 % of women before menopause, most often in the third decade of life. In the mildest form, the pain lasts only a few days prior to menstruation. The number of symptomatic days varies, however, and a few women can experience pain for virtually the whole month, with relief occurring only at the time of menstruation.
In approximately 10 % of these women, pain will be severe and interfere with their normal activities. A minority of women with the most severe pain will also experience it during menstruation. The pain can continue for many years but will usually disappear after menopause. In 20 % of women, it subsides without any intervention.
Cyclic mastalgia includes pain varying with menstrual cycle as well breast pain in women without periods but with ovarian function (i.e. post hysterectomy) or even postmenopausal ones taking hormone replacement therapy (HRT). Many women describe the pain as dull, burning, throbbing or aching, usually starting in the upper quadrant of the breast. Sometimes a shooting pain radiating to the arm and axilla may be present, probably secondary to glandular pressure on the intercostobrachial nerve (Fig. 7.2).
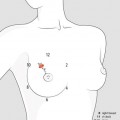
Fig. 7.2
Symptoms and localisations of cyclical mastalgia. Symptoms may include a dull ache, heaviness, tightness, a burning sensation or breast tenderness. Pain is brought on by activity and may be reproduced by pressure on the upper outer quadrants, often associated with nodularity, radiated down the arm and toward the axilla, and relieved by menstruation [3, mod. with permission.]
Even though both breasts can be involved, patient often claim one breast is worse than the other. On clinical examination, diffuse tenderness with lumpiness and nodularity in the breast is detected when the pain is present, and the upper outer quadrants of the breast are most commonly affected. There is no single discrete lump to feel and there are no abnormalities with the nipple. Mammography typically shows no abnormality, but the breast tissue can appear glandular and dense.
7.3 Noncyclic Mastalgia
Clinical Practice Points
In noncyclic mastalgia, the pain in the breast is not related to the menstrual cycle and shows broad patterns and a poorer response to treatment.
If any cause for chronic, severe and persistent breast pain is found, noncyclic mastalgia should be considered idiopathic.
In some cases, differential diagnosis of overlapping symptoms of true noncyclic mastalgia and non-mammary pain turns out to be challenging.
Patterns of noncyclic mastalgia are: ill-localised pain not associated with menstrual periods. Symptoms usually are unilateral, involve upper quadrants and are described as heavy, aching, tender, concerning, burning, pulling, stabbing and pinching. True, or idiopathic, noncyclic mastalgia should be differentiated from breast pain due to specific pathologies as periductal mastitis or fat necrosis. Sometimes symptoms are so undistinguished that a challenging diagnosis with non-breast pain should also be done (Fig. 7.3).
Fig. 7.3




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
