Fig. 34.1
Preoperative view. The 49-year-old patient was scheduled for a quadrantectomy (B plasty) for invasive cancer of the left breast and excision of a fibroadenoma of the right breast
Reoperation surgery was done with wide re-excisions on the left breast and a B plasty quadrantectomy on the right breast.
Histology of both specimens again revealed involved margins. Due to a positive family history (no mutation defect found in genetic testing), an otherwise unsuspicious mammogram (no microcalcifications, no masses in the radiological examinations), and a poor cosmetic outcome after bilateral quadrantectomy and re-excision, the patient decided for a bilateral mastectomy and immediate reconstruction with implants. Following multiple previous surgeries, the patient revealed two small non-ptotic breasts with scars from the B plasties (Fig. 34.2a–c).
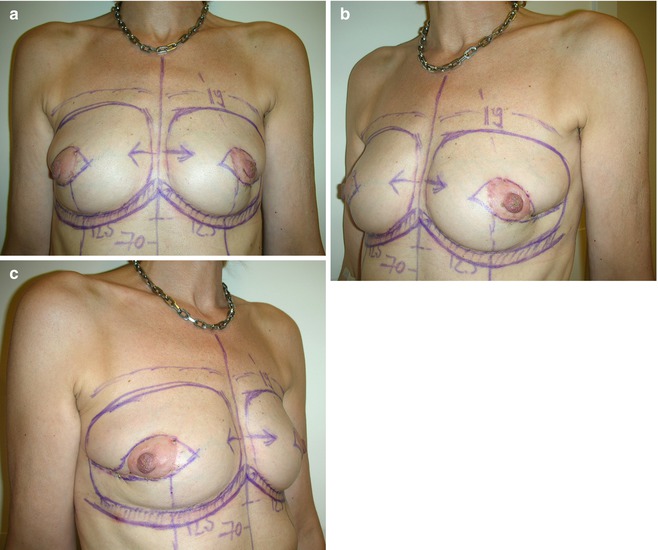
Fig. 34.2
(a–c) Following B plasty and re-excision on the left breast and tumorectomy and B plasty for incidentally found cancer on the right breast, the patients showed small non-ptotic breasts with scars after bilateral B plasties. A tissue deficit was seen in the lateral quadrants of both breasts with the nipple position too far laterally. Drawings were made for bilateral skin-sparing mastectomy and immediate reconstruction with implants
34.2 Surgery
A bilateral skin-sparing mastectomy was performed. The resection of the nipple-areola complex (NAC) was done due to the preference of the patient, the extensive intraductal carcinoma, and the uncertain blood supply of the NAC when a nipple-sparing mastectomy is performed after a B plasty. Sentinel node biopsy found two nodes in each breast, which were negative in the frozen-section examination. Immediate reconstruction was done with 250 cc anatomical implants inserted in the subpectoral pocket (Fig. 34.3a, b
 Doughnut Lumpectomy: Caveat II
Doughnut Lumpectomy: Caveat II
 Doughnut Lumpectomy: Caveat I
Doughnut Lumpectomy: Caveat I
 Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
 Defect Reconstruction After Breast Conservation Surgery and Radiation with Lipofilling
Defect Reconstruction After Breast Conservation Surgery and Radiation with Lipofilling
 Correction of a Postlumpectomy Deformity Scar by Lipofilling
Correction of a Postlumpectomy Deformity Scar by Lipofilling
 Nipple-Areolar Complex (NAC) Reconstruction: Good Case
Nipple-Areolar Complex (NAC) Reconstruction: Good Case




Related posts:
Doughnut Lumpectomy: Caveat II
Doughnut Lumpectomy: Caveat I
Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
Defect Reconstruction After Breast Conservation Surgery and Radiation with Lipofilling
Correction of a Postlumpectomy Deformity Scar by Lipofilling
Nipple-Areolar Complex (NAC) Reconstruction: Good Case
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
