12 Body Peeling
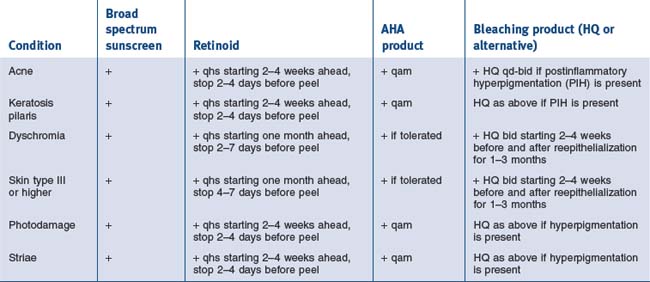
When discussing the approach to chemical peeling off the face, adjectives such as conservative and gradual should come to mind. Common indications are much the same as their facial counterparts and can be grouped into those that would be best treated with superficial peels and those that would benefit from medium-depth peels (see Table 12.1).
Table 12.1 Indications for superficial and medium-depth peels
| Superficial peels | Medium-depth peels |
|---|---|