(1)
University of Pittsburgh Medical Center, Pittsburgh, PA, USA
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-662-46976-7_5) contains supplementary material, which is available to authorized users.
5.1 Background
When operating on males after massive weight loss (MWL), plastic surgeons are understandably concerned with the demands of correcting ptotic gynecomastia, hanging pannus, oversized flanks, and ptotic mons pubis, and buttocks (Fig. 5.1). The patients may also request reduction of excess skin and fat of the arms and thighs. While these localized problems demand skin and fat excision, the overriding issues for many men are reducing lower torso fullness and enhancing visibility of superficial muscles. That physique is accomplished by tightly closing skin with thin subcutaneous tissue over well-developed muscles.

Fig. 5.1
A 26-year-old, 6′, 215 lb androgynous-appearing male dominated by gynecomastia and larger lower body. Well-shaped ptotic breasts are supported by a well-defined IMF. He has a large pannus overhanging his groins and mons pubis. His flanks are widely bulging
Not so in women, where the finesse in body contouring is sculpturing adipose-related curvatures of the breasts, hips, buttocks, and thighs (Chap. 4). Since plastic surgeons operate on women more than 80 % of the time (Chong et al. 2012), misguided efforts in males is understandable. Inferior buried pedicle flaps for correction of pseudogynecomastia (Gusenoff et al. 2008) and bikini level lower body lift incisions (Lockwood 1996) are two examples of misapplying approaches for female to male surgery. Those techniques and others fail to accentuate muscularity and upper body dominance.
Instead of gender esthetics, variances to females in preoperative presentation and postoperative complications are the focus of a recent review of 48 male MWL contouring body patients (Gusenoff et al 2008). Men present with a greater change in BMI and less clinical depression than women. Forty-two percent overall complications, mostly hematomas and seromas, was statistically greater than females. Advanced techniques in liposuction of the muscular male torso have become more sophisticated than excisional surgery. Etching of the male torso (Hoyos and Millard 2007; Mentz et al. 2007) has advanced to 4-dimensional VASERlipo of subcutaneous adipose along with lipoaugmentation of superficial muscles (Hoyos and Perez 2012).
Comprehensive surgery in males is demonstrated through a variety of case presentations. The cases are numbered and listed with operations at each stage and the reason for their inclusion (Table 5.1). All the cases have before images with and/or without preoperative surgical markings and an identical set of afters.
Table 5.1
Demonstrative case presentations
Case | Operation | Lessons |
|---|---|---|
5.1 | VASERlipo of torso | Markings, defining VASERlipo without excisions |
5.2 | Boomerang/transverse UBL/UAL | Markings, simple gynecomastia excision/UBL with UAL in overweight |
5.3 | Boomerang/J-torsoplasty | Delayed 2nd-stage TBL, markings, intraop. video |
5.4 | Boomerang/J-torsoplasty | Delayed 2nd-stage TBL, markings, year result |
5.5 | Boomerang/J-torsoplasty | Markings, successful secondary surgery after failed two stages |
5.6 | Single-stage TBL, transverse lifts | Transverse markings, lower body deformity, VASER correction |
5.7 | Single TBL, oblique excisions | Markings, intraoperative, excellent early result |
5.8 | Single TBL, oblique excisions | Additional preop weight loss, markings, excellent 2-year result |
5.9 | Single TBL, oblique excisions | Excellent result at 2 years with thickened medial chest scars |
Advances in superficial liposuction and lipoaugmentation have incredibly enhanced muscular show in the average body builder.
5.2 VASERlipo to Enhance Muscular Show in Case 5.1
With the increased specificity for fat extraction and safety of VASERlipo (Sect. 3.2.7), aggressive superficial sculpture liposuction is applied to improve muscular show and enhance the upper bodies in males.
5.2.1 Case 5.1 VASERlipo of Torso
Case 5.1 is a 44-year-old frustrated male recreational body builder. He distains his gynecomastia, submental fullness, and generalized lack of muscular show. He has no loose skin. He was marked blue on his neck and torso for liposuction, black for etching depths, and green for lipoaugmentation (Fig. 5.2). Red marks indicate no treatment. The operation was started prone. After infusion of 4,200 cc of saline with xylocaine and epinephrine, 3-ring VASER probe was applied at 80 % VASER mode for 44 min to the back and flanks through stab incisions in the lower lumber midline, posterior Iliac crests, upper back, and arm back junction. The midline of the back was deeply etched. The liposuction through 3 and 3.7 mm diameter VenTx low-pressure cannulas delivered into the Harvester jar 900 cc of emulsion from the flanks and lower back, 600 cc from upper back and 175 cc from each arm. Excess fluid was decanted. The remaining emulsion was strained through a colander. 100 cc of particulate fat was injected within the green zone of each buttock. After he was turned supine, the process was repeated. 1,400 cc saline was injected into the anterior torso, and then after VASER application for 30 min, 1,400 cc of emulsion was extracted. As marked in black, the rectus abdominis inscriptions, the lateral and inferior pectoralis muscle adherences, and the costal groove were accentuated by deliberate oversuctioning beveled depressions with high-vacuum 3 mm cannula. His gynecomastia was completely aspirated, obviating the need for a pull-through resection of gland. 175 cc of aspirated and filtered fat is injected into each pectoralis major muscle and 40 cc into each deltoid muscle. One year later, his gynecomastia has been corrected with no nipple or glandular ptosis (Fig. 5.3). Excess fat has been removed from his neck and throughout his torso. All his torso superficial muscles are better defined along with highlighted skin adherences. His fat-grafted central buttocks and pectoralis and deltoid muscles are esthetically fuller. The abdominal and back midlines are deeply defined. The upper body is dominant.
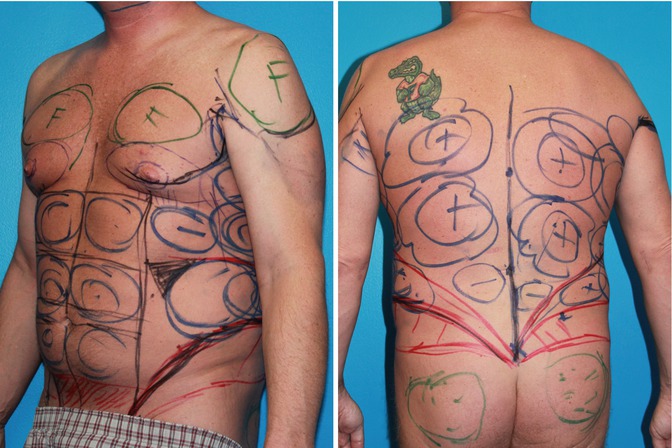

Fig. 5.2
Case 5.1. High-definition VASERlipo for frustrated weight-lifting 34-year-old male. He has no muscular definition or upper body dominance. Markings for VASERlipo for generalized reduction of excess adipose, correction of gynecomastia, and then definition of his muscles. Blue is for general liposuction, black for contour highlights, and green for augmentation of the pectoralis and deltoid muscles and buttocks. 3,200 cc of fat was removed. 175 cc were added to each pectoralis major muscle, 40 cc to each deltoid, and 100 cc to each buttocks. Red marks indicated no suctioning
Fig. 5.3
Case 5.1 result 1 year later shows absent gynecomastia, defined muscles with fuller buttocks, and pectoralis and deltoid muscles. Depressed midlines accentuate the V-shaped torso
In addition to adipose, the remaining men in Chapter 5 have both horizontal and vertical skin excess, which requires excisional procedures to reveal underlying muscles.
5.3 Goals, Analysis, and Planning
When there is redundant torso skin, whether it is through massive weight loss (MWL) or aging, it is mostly but not all vertical. Transverse excision is effective but incomplete since some horizontal skin excess remains. For the tightest result, the residual horizontal excess needs to be removed vertically. For optimal muscular show, the skin with thin subcutaneous layer needs to be tightly wound, and therefore, skin is removed in both the vertical and horizontal planes.
Common examples of removing excess skin in both horizontal and vertical planes are the fleur-de-lys abdominoplasty (FDL) and the Wise pattern breast reduction. Vertical excisions and resulting scars are an accepted but unesthetic tradeoff for removing excess horizontal skin. The FDL leaves a conspicuous scar from xyphoid to pubis and a coverable crossing scar across the groins. While a wide midline abdominal vertical excision effectively removes central horizontal skin laxity and a narrower waist, there is understandable reluctance to trade mild to moderate skin laxity for that vertical long scar. When a midline surgical scar is already present, then an FDL can be an excellent choice. The Wise pattern breast reduction leaves a visible vertical scar from nipple to inframammary fold (IMF) and a hidden scar along the IMF. Fortunately that short vertical scar across the central lower pole of the female breast tends to heal thin. When applying the Wise pattern to MWL gynecomastia (Gusenoff 2008), the vertical excision of horizontal excess is also limited to between the NAC and the inframammary fold (IMF). Not only does that limited vertical excision leave excess horizontal skin over most of the pectoralis muscle but also that vertical scar in men is obvious. When the nipple is then transposed on an inferior-based deepithelialized flap, undesirable fullness is added between the nipple and the new IMF. Upon contraction of the pectoralis muscle, that fullness prevents customary emptying inferior to the nipple, thereby distorting dynamic anterior chest esthetics. The Wise pattern horizontal closure is design to be the new IMF, which is an undesirable anatomical adherence in men.
While effective to remove horizontal skin excess, a long vertical excision along the breast meridian would leave an unacceptable clavicle to costal margin scar. A compromise is removal of both horizontal and vertical skin excess through complimentary series of wide oblique excisions across the central chest (Fig. 3.2). It has been our experience and others (Letterman and Shurter 1972) that obliquely oriented chest scars heal most favorably. The concept to expose underlying muscular definition through connected oblique excisions began in the chest (Hurwitz 2004). Gynecomastia along with redundant chest skin is corrected by removal of all excess upper body chest skin and direct or liposuction removal of the breast gland through a long undulating excision and obliteration of the IMF. With the advent of the J-torsoplasty (Clavijo-Alvarez et al. 2012) for the mild to moderate back laxity, the transverse upper body lift with its scar winding around the back became obsolete. Furthermore, this midlateral chest torsoplasty removes lateral chest bulk and further tightens the anterior chest skin for improved definition of the lateral borders of the pectoralis major and latissimus dorsi muscles.
Lower body lifts (LBL) that hug the pelvic rim best efface saddlebag deformity and provide deepithelialized adipose fascia flaps for buttock augmentation. Those attributes are lost when more superior oblique flaps are used. Unfortunately, low-lying LBL incompletely correct bulging flanks and were frequently complicated by lateral gluteal contour depressions. Furthermore, deepithelialized hairy buttock flaps are prone to chronic seromas and sinus tracks. Direct flank excision through long oblique posterior extensions of the abdominoplasty leave a deeper tight-skinned waist. Hence, in 2008, the transverse upper and lower body lifts were replaced by J-torsoplasty and oblique posterior extensions of the abdominoplasty directly over the bulging flanks (Hurwitz 2014) (Fig. 3.2).
With excess skin, optimal results are obtained when the subcutaneous depth is evenly thin, and both horizontal and vertical excess is excised across the entire torso. This is performed through an excision pattern, leaving unobtrusive scars and low risk of complications. Additional contouring through liposuction or lipoaugmentation is considered then or at a later stage.
Surgical enhancement of masculinity starts with an analysis of skin and adipose excess along with the impact of the musculoskeleton on the patient’s surface typography. Men who have expanded to gigantic proportions and then lost hundreds of pounds should be examined for a distorted musculoskeleton that thwarts esthetic goals. Massive barrel chest, kyphosis, widened pelvis, and oversized muscular thighs are impediments to esthetic success. Inadequate weight loss or partial regain leaves generalized excess fat that would obscure muscularity. Further preoperative weight loss until the nonresected areas are thin enough is best. Alternatively, secondary liposuction is beneficial.
A typical presentation is MWL patient in Fig. 5.1 with an inverted body. His bulging flanks are wider than his shoulders. He has projecting gynecomastia overhanging well-defined IMFs. Slightly large NACs aglie below pectoral muscles. The adipose fullness extends across the lateral chest to his latissimus dorsi muscles. His pectoralis muscle is full with a muted lateral pectoral roll. The chest and upper abdomen exhibit loose skin. Despite a hanging abdominal pannus, there is linear concave contour definition along the midline between his rectus abdominis and oblique muscles. His buttocks are round. The lateral border of the latissimus dorsi muscle is obscure. His bulging flanks extend over his iliac crests to widen his hips. His midline anterior chest and entire posterior are normal. His TBL surgery is presented after a discussion of isolated boomerang correction of gynecomastia.
5.4 Boomerang Pattern Correction of Gynecomastia
Gynecomastia is the development of a female-appearing breast on a man. It is a common clinical problem, classified by severity. If the etiology is not endocrine or drug related, surgery is the treatment. Fat and glandular tissue needs to be excised. Excess skin may be allowed to retract or if necessary be resected in a variety of skin patterns, keeping the scar length to a minimum. Gynecomastia after MWL is a subset population of breasts surrounded by sagging midtorso skin. These patients require comprehensive evaluation and treatment to eliminate the gynecomastia while reshaping the torso.
While the breasts are large in the obese, gynecomastia after MWL tends to have mild to moderate excess volume and ptosis. When the skin laxity of the gynecomastia approximates the midtorso laxity, these patients require a comprehensive approach. A more limited approach only to the breast is appropriate when the gynecomastia is very severe. In those instances, the objective is to remove large and sagging breasts and establish a proper nipple position with as few scars as possible. Similarly, men who do not exhibit much chest skin laxity or prefer their laxity to a long undulating chest scar are not candidates for this comprehensive surgery.
5.4.1 Case 5.2 Boomerang/Transverse UBL with UAL
In Case 5.2, complimentary obliquely oriented ellipses draping over the nipples were drawn to capture both horizontal and vertical excess skin (Fig. 5.4). The 90° orientation of the ellipses capped by a dome that bridges the current to new location of the superior rim of the NAC effectively removes excess anterior chest skin in both the vertical and transverse axes. The long scar is broken up by the NAC and usually fades over time (Fig. 5.5). The skin redundancy caused by extensive torso ultrasound-assisted lipoplasty (UAL) was absorbed by the boomerang/transverse upper body lift excision. As seen in the preoperative markings and the yellow overlay in Fig. 5.4, the smaller ellipse starts roughly at the lowest costochondral sternal junction and rises to across the planned raised NAC cutout. The larger second elliptical excision rises from about the 7th rib at the anterior axillary line to meet the smaller ellipse at roughly right angles at the new NAC. In these initial cases, the lateral ellipse is extended transversely across the back for the upper body lift. This unique asymmetrical excision, which encircles 60 % of the NAC, is called a boomerang pattern because of its likeness to the Australian weapon. The remaining surgical markings in Case 5.1 consists of pluses within large circles indicative of quantity of planned ultrasound-assisted lipoplasty (UAL) of the entire trunk in this 240 lb, 6′ male. This gynecomastia correction is associated with 4,000 cc UAL of the trunk, which would have left loose skin if not for the wide skin resections. The result 2 years later in this relatively simple case shows satisfactory correction of the gynecomastia and no loose skin of the trunk (Fig. 5.5).
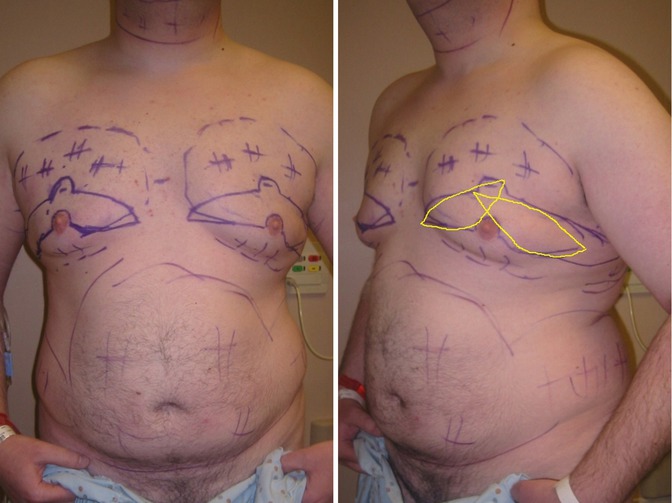

Fig. 5.4
Case 5.2 Frontal and lateral views of 6′ 2″, 240 lb, 32-year-old male is marked for UAL of the trunk and boomerang pattern correction of gynecomastia with short transverse extensions around to the back. The yellow overlay ellipses are not the excision patterns but the essential geometry that raises the NAC and removes excess skin in both the horizontal vertical planes. The nipple areolar complex is based on a broad inferior pedicle. The planned elevation of the NAC is superior to the inferior lateral adherence of the pectoralis major muscle. Within large circles are pluses to indicate relative quantities of fat to be extracted by UAL
Fig. 5.5
The frontal and lateral view of Case 5.2 two years after a boomerang correction of gynecomastia with transverse extensions and 4,000 cc of fat suctioned from the torso. There is smooth reduction of the subcutaneous fat and absence of the gynecomastia with tight skin, reflecting underlying muscularity. The extensive scar, interrupted by the nipples has faded
5.4.2 Case 5.3 Boomerang Gynecomastia with J-Torsoplasty
The boomerang pattern correction is usually combined with a J-torsoplasty. Case 5.3 demonstrates through photographs and Videos 5.1, 5.2 the current management of multiple upper torso rolls and gynecomastia after MWL. He is a 6′ 6,″ 210 lb 24-year-old male requesting total body contouring (Fig. 5.6). Obese in childhood, he lost 175 lb in college. He has a distinct set of back rolls at the lateral breasts, around the mid torso and the flanks. In the first stage, an abdominoplasty with oblique extensions over the flanks removed lower torso excess. The result of stage-one lower body surgery is seen 2 years later when he is marked for his upper body surgery (Fig. 5.7, left). The lower abdominal and flank excess and bulge have been corrected. The scar is symmetrical, flat, and mildly hyperpigmented. There is mild adipose-glandular fullness under his ptotic lower pole and NACs. As a muscular male, he desires correction of his gynecomastia and skin tight covering over his pectoralis muscles. He wants no epigastric, mid-back, and lateral breast rolls. He accepts a long zigzag scar pattern of an upper body lift but prefers no additional back scars.
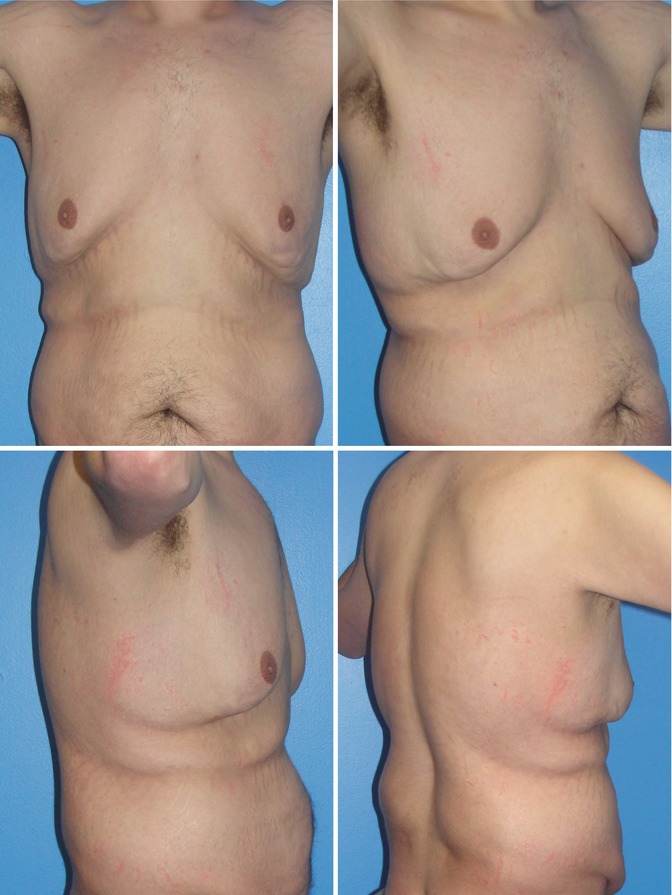
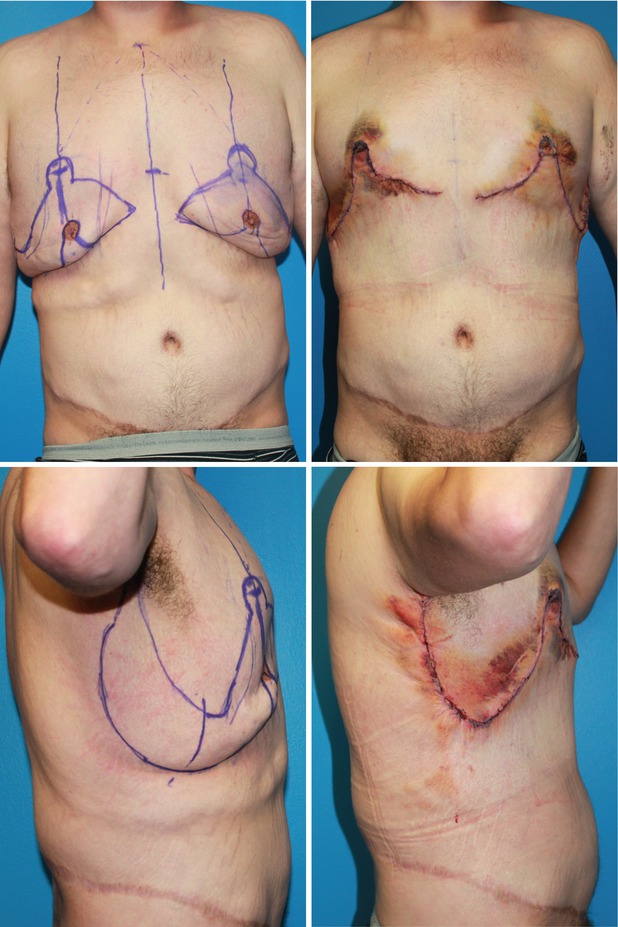
Fig. 5.6
Case 5.3. 6′ 6″, 210 pounder presents for gynecomastia correction and TBL after losing 220 lb. His androgynous form has diffuse sagging skin with moderately severe gynecomastia
Fig. 5.7
Case 5.3 Preoperative markings and early result from second-stage boomerang correction of gynecomastia with J-torsoplasty. Two years after successful abdominoplasty and LBL, Case 3 is marked for the second-stage TBL consisting of boomerang pattern correction of his gynecomastia with a J-torsoplasty extension (left). Ten days later, at the time of his last office visit, the healing closure is tight (right)
The companion video shows the marking and surgery for a boomerang correction with a J-torsoplasty. The early result shows excellent healing, chest contour, and NAC position (Fig. 5.7, right




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
