, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
29.1 Accessory Tragus
29.1.1 Clinical Features
Accessory tragus is a common congenital abnormality of the external ear with prevalence of 1–10 per 10,000 live births and bilateral involvement in 6 % of cases [1, 2]. No gender or racial predilection exists. Accessory tragi are skin-colored, soft, polypoid papules that occur along an arc on the preauricular cheek and extending from the tragus to the angle of the mouth and the anterior margin of the sternomastoid muscle (Fig. 29.1). Lesions typically are solitary but may be multiple or bilateral. When located along the neck, lesions may be qualified as a “wattle,” a cartilaginous rest on the neck of cervical accessory tragus. Most cases of accessory tragus occur in isolation, but some have been reported as a feature in some genodermatoses with additional anomalies involving the first and second branchial arches.

Fig. 29.1
Two skin-colored papules on the preauricular skin represent accessory tragi
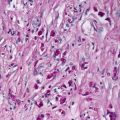
29.1.2 Histology
The histologic appearance of an accessory tragus is that of a polypoid lesion with thin epidermis. The dermis is remarkably thin with subcutaneous fat very close to the epidermis (Fig. 29.2). Abundant vellus hairs are present throughout the hamartoma (Fig. 29.3). There is no cytologic atypia, and all elements of the skin appear fully mature. Cartilage is present in only a minority of cases and is not required to establish the diagnosis when the other histologic criteria are present in the appropriate clinical setting.

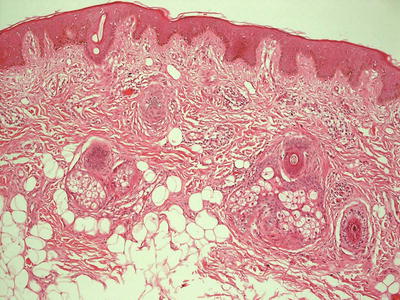
Fig. 29.2
Abundant vellus hairs, ectopic cartilage, and fat located high in the dermis are present in an accessory tragus
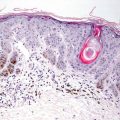
Fig. 29.3
The diagnosis of an accessory tragus can be made based upon clinical presentation, abundant vellus hairs, and superficially located fat within the dermis even in the absence of ectopic cartilage
An acrochordon is in the differential diagnosis, but the presence of subcutaneous fat close to the epidermis and abundant vellus hairs helps in resolving the dilemma. When cartilage is present, the diagnosis is straightforward.
29.1.3 Pathogenesis
Accessory tragus is a common benign congenital malformation of the first and second branchial arches. During early embryonic development, hillocks, which are soft tissue swellings on the surface of the embryo derived from the first and second branchial arches, are formed. The hillocks grow and fuse to form the helix, antihelix, and tragus. Abnormalities that occur during this process can result in the formation of an accessory tragus. Interestingly, accessory tragus may be a sign of other syndromes, such as oculoauricularvertebral syndrome (Goldenhar syndrome ) [3].
29.2 Supernumerary Nipple
29.2.1 Clinical Features
Polythelia or supernumerary nipple is the most common anomaly on the breast in children with reported incidence of approximately 5 % [4, 5]. Occurrence usually is sporadic. Supernumerary nipple presents as a hyperpigmented papule, which may be atrophic/concave or exophytic, along the embryologic milk lines at the anterior torso (Fig. 29.4). Less commonly, they can occur on the face, neck, shoulder, back, genitals and thighs [4].