Basic dermatological surgery
The demand for the removal of benign and malignant skin lesions has increased considerably, such that skin surgery is now practised by many general practitioners as well as by dermatologists. Knowledge of basic surgical techniques is mandatory for all those who treat skin disease.
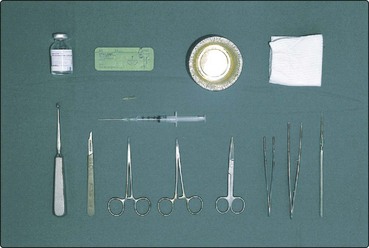
Instruments and methods
The basic instruments (Fig. 1) include a #3 scalpel handle and #15 blade, a toothed Adson’s forceps, a small smooth-jawed needle holder, a pair of fine scissors, artery forceps and a Gillies skin hook. Curettes and skin punches come in various sizes. A solution of 1% lidocaine (Xylocaine) with 1/200 000 adrenaline (epinephrine) is usually satisfactory as the local anaesthetic, but plain lidocaine must be used on the fingers, toes and penis. The maximum safe dose for an 80-kg person using 1% lidocaine and adrenaline (1/200 000) is 40–50 mL. This volume is significantly reduced if higher concentrations of lidocaine or no adrenaline are used. The skin is prepared (but not sterilized) using, for example, 0.05% aqueous chlorhexidine (Unisept). Alcohol-based preparations are avoided as, if cautery is used, the solution may ignite. Sterile towels, placed around the operation site, reduce the chance of infection.
Basic surgical techniques
Excisional biopsy
An excisional biopsy is planned after considering the local anatomy. The excision’s axis depends on the skin creases (Fig. 2) and its margin on the nature of the lesion. The ellipse to be excised is drawn on the skin using a marker pen. An ellipse has an apical angle of about 30° and is usually three times as long as it is wide. If any shorter, ‘dog-ears’ appear at either end, although these can easily be corrected. After cleaning, local anaesthetic is infiltrated using a fine needle into the area of the lesion. Once numbed, the skin is incised vertically down to fat with the scalpel, in a smooth continuous manner to complete both arcs of the ellipse. The ellipse is freed from surrounding skin, secured at one end with a skin hook and removed from the underlying fat, usually using the scalpel blade (Fig. 3). In most cases, the wound can now be repaired, although any bleeding vessels will need to be stemmed with cautery, hyfrecation or suturing.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


