, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
11.1 Toxic Shock Syndrome
11.1.1 Clinical Features
The sudden development of shock and organ failure in an otherwise healthy person with an intact immune system is frequently caused by a wide variety of primary infections with Streptococcus pyogenes or Staphylococcus aureus .
Cases of streptococcal toxic shock tend to be sporadic with a prevalence of 10–20 per 100,000 individuals. Mortality is estimated at 30–70 % [1]. Up to 90 % of staphylococcal toxic shock cases occur in females, and more than 90 % affect Caucasian females between 15–19 years of age [1]. In the case of a primary soft tissue infection with either pathogen, there is often swelling, redness, and pain at the site. Deeper infectious processes may result in frank bullae on the skin. In addition to systemic symptoms of fever, hypotension, tachypnea, and tachycardia, patients typically develop a diffuse or patchy erythematous rash resembling a sunburn . Mucous membranes may appear erythematous, and there may be a “strawberry” tongue. Patchy superficial desquamation is common about 7–14 days after onset of the illness. Some patients experience transient patchy alopecia or temporary loss of nails.
11.1.2 Histology
Histologic changes unique to children have not been described. The changes include focal spongiosis with small neutrophilic abscesses within the epidermis, along with clusters of dyskeratotic keratinocytes [2] (Figs. 11.1 and 11.2). Within the dermis , there is a mixed inflammatory infiltrate with lymphocytes, neutrophils, and eosinophils, both interstitially and around vessels. In some cases, the pattern resembles a leukocytoclastic vasculitis, but fibrin thrombi are absent [2]. Papillary dermal edema and focal hemorrhage are variably present.
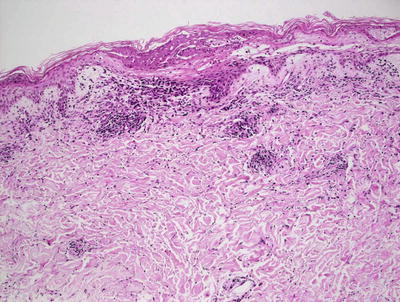
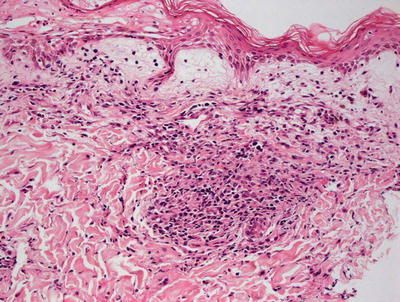
Fig. 11.1
A lymphocytic infiltrate is seen underneath a necrotic epidermis in toxic shock syndrome
Fig. 11.2
Necrotic epidermis is seen overlying papillary dermal edema and a mild perivascular lymphocytic infiltrate in toxic shock syndrome
11.1.3 Pathogenesis
Toxic shock syndrome is primarily caused by Staphylococcus aureus with fewer reports seen in patients with group A streptococcal infection [1]. While most cases are associated with tampon use during menstruation, other exposures to bacterial colonization may be present in up to 13 % of cases [3]. Following bacterial colonization, toxic shock syndrome toxin type 1 is produced. In rare instances, staphylococcal enterotoxins A-H have been implicated in the disease. Most adults have developed antibodies to these exotoxins, and are relatively resistant to the disease. However, those without sufficient immunity, as well as those with altered levels of serum glucose or magnesium, may be at increased risk. Exotoxins cause tissue destruction through stimulating interleukin 1 (IL-1) and tumor necrosis factor. T lymphocytes are also stimulated and contribute to symptoms of shock and tissue destruction.
11.2 Blastomycosis-Like Pyoderma
11.2.1 Clinical Features
Blastomycosis-like pyoderma is a condition that primarily affects middle-aged individuals with a male-to-female ratio of 3:1 [4]. Although the etiology is unknown, it is thought to represent an exaggerated, chronic inflammatory reaction in the skin, possibly with an infectious component.
The classic skin lesions start as erythematous papulopustules that coalesce into vegetative verrucous plaques with raised borders. They are most common on the face, scalp, axillae, and genitalia, but may also affect the abdomen, trunk, or distal extremities. Oral lesions have been reported and present as white pustules or plaques. Although lesions occasionally heal spontaneously, they tend to be chronic and recurrent. There are no standard treatment recommendations; some cases improve with wound care, systemic antibiotics, and treatment of any underlying systemic disease process (e.g., inflammatory bowel disease).
11.2.2 Histology
Histologic features of blastomycosis-like pyoderma include florid epidermal hyperplasia that is pseudoepitheliomatous in some cases. A neutrophilic infiltrate is present as abscesses within the stratum corneum, epidermis, and dermis [5]. In florid cases, disruption of follicular units may result in marked diffuse dermal inflammation that can be predominantly neutrophilic or granulomatous. Tissue gram stains may or may not demonstrate microorganisms, but tissue cultures are invariably positive for bacterial growth.
The histologic differential diagnosis includes infectious etiologies, such as deep fungal and mycobacterial infections, as well as halogenodermas and squamous cell carcinoma . Stains for microorganisms may help with this distinction, and tissue cultures can definitively resolve the differential diagnosis with the other infectious etiologies. Halogenodermas tend to have abundant eosinophils that are not characteristic of blastomycosis-like pyoderma. Keratinocyte atypia is more pronounced in most cases of squamous cell carcinoma than the reactive squamous atypia seen in some cases of blastomycosis-like pyoderma. An infiltrative growth pattern seen in squamous cell carcinoma is also not seen in blastomycosis-like pyoderma.
11.2.3 Pathogenesis
The disease is almost always induced by bacterial infection, most commonly Pseudomonas and Staphylococcus [6]. There is a single report of a case caused by Trichophyton mentagrophytes [7]. Blastomycosis-like pyoderma is believed to be a hypersensitivity reaction occurring in patients with altered immunity [6, 8]. Impairment of both systemic and local immunologic responses has been associated with this reaction pattern [5].
11.3 Chronic Granulomatous Disease
11.3.1 Clinical Features
Chronic granulomatous disease is a rare primary immunodeficiency. Patients often present in early childhood with symptoms of inflammatory bowel disease and recurrent unusual opportunistic infections. Development of widespread infectious and noninfectious granulomas is common. Skin manifestations include soft tissue infections with formation of abscesses and ulcers. These are often caused by uncommon microorganisms, such as Serratia marcescens [9].
11.3.2 Histology
Histologic findings vary depending upon the presence of superinfection. Most cases demonstrate the presence of granulomatous inflammation within the dermis. A characteristic golden-yellow pigmented lipid has been described within giant cells in the granulomatous reaction, especially at the periphery of lesions [10]. This is believed to be a degenerative bi-product of the defective abilities to destroy microorganisms. If there is an active secondary infection, the presence of neutrophils is an expected finding. In some cases, neutrophils may occur as intraepidermal vesicles or dermal abscesses [10]. In patients without current infection, a nonspecific lymphohistiocytic infiltrate may be present [11]. Tissue cultures are usually negative.
11.3.3 Pathogenesis
Chronic granulomatous disease is caused by a one of five genetic defects that result in impairment in phagocyte NADPH oxidase [12]. Functioning phagocyte NADPH oxidase generates reactive oxygen species that are involved in extracellular host defense, and are essential for fully resolving inflammatory processes. Defective oxidase function results in an ineffective respiratory burst in phagocytes that cannot effectively destroy certain bacteria and fungi [13].
11.4 Impetigo
11.4.1 Clinical Features
Impetigo is a common cutaneous infection with high prevalence in children. Non-bullous or “crusted” impetigo accounts for more than 70 % of the cases [14]. It affects children and adults, but is rarely seen in children under 2 years of age. It can be caused by group A ß-hemolytic streptococci and Staphylococcus aureus. The primary lesion is a superficial vesicle, which ruptures easily, leaving an erythematous erosion and purulent exudate that quickly dries and form the classic “honey colored” crust (Fig. 11.3).

Fig. 11.3
Impetigo presents as widespread flaccid bullae and superficial erosions with collarettes of scale and foci of honey-colored crust (photo courtesy of Minh Hoang, MD, Ho Chi Minh City, Vietnam)
The bullous form of impetigo is most common in children between 2 and 5 years of age. It is nearly always caused by S. aureus infection. It presents as superficial flaccid vesicles and bullae that rupture easily, leaving erythematous erosions with “collarettes of scale” behind. Although bullous impetigo can occur on any cutaneous surface, it is somewhat more common in moist intertriginous areas. Most localized forms of impetigo can be treated with topical antibiotics. More extensive cases or cases with systemic symptoms, such as fever, are treated with systemic antibiotics.
11.4.2 Histology
Histologic sections demonstrate a subcorneal neutrophilic pustule (Fig. 11.4). There is spongiosis within the epidermis, and a variably intense inflammatory infiltrate within the dermis. Focal acantholysis may be seen in some cases. Neutrophils may be present throughout the epidermis and focally in the dermis (Fig. 11.5). In older lesions, a thick crust with serum and parakeratosis is seen. Tissue Gram stains will demonstrate gram-positive cocci, most commonly Staphylococcus and less commonly Streptococcus.
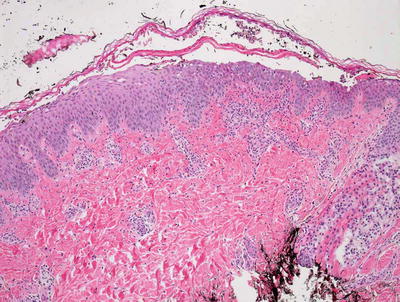
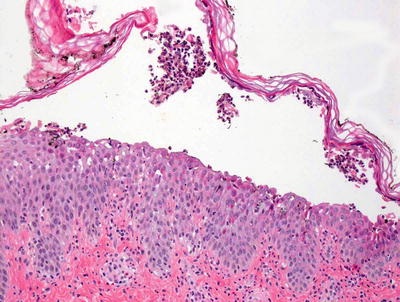
Fig. 11.4
Bullous impetigo displays a subcorneal neutrophilic abscess
Fig. 11.5
Neutrophilic abscesses and scattered neutrophils within the epidermis and superficial dermis are seen in bullous impetigo
The differential diagnosis includes other subcorneal blistering disorders, such as candidiasis, transient neonatal pustular melanosis, erythema toxicum neonatorum, acute generalized exanthematous pustulosis (AGEP), and acropustulosis of infancy. All of these entities do not demonstrate bacterial infection. In candidiasis, a PAS stain will show fungi. Erythema toxicum neonatorum is characterized by a predominantly eosinophilic pustular infiltrate as opposed to the neutrophil predominant infiltrate seen in impetigo. The other entities are best distinguished based upon the clinical presentation and history as there is no clinical overlap with impetigo.
11.4.3 Pathogenesis
Exfoliatin toxin is strongly implicated in the pathogenesis of bullous impetigo associated with staphylococcus aureus infection [15]. Likewise, exfoliative toxin A-coding bacteriophages are identified in most cases of impetigo [16]. Group A β-hemolytic streptococcal strains are also the cause of impetigo, although they are less commonly reported [14].
11.5 Scarlet Fever
11.5.1 Clinical Features
Scarlet fever is caused by infection with toxin-producing strains of group A β-hemolytic streptococcus . Most cases affect children between 1 and 10 years of age, although it is occasionally seen in older children and adults [17]. Fever, pharyngitis, and a diffuse erythematous rash characterize scarlet fever. Pinpoint erythematous macules and papules coalesce into a diffuse sunburn-like erythema with a rough, “sandpaper” texture. There is accentuation of erythema with transverse red streaks in the skin creases (“Pastia’s lines”). The tongue appears red and swollen with prominent papillae (“strawberry tongue”).
11.5.2 Histology
Scarlet fever is almost always diagnosed based upon clinical findings and serologic studies. The histologic findings are nonspecific, but include dilated and congested dermal blood vessels. Edema and hemorrhage have been described, often accompanied by a slight infiltrate of neutrophils. Late stage lesions demonstrate parakeratosis that can be diffuse and confluent.
11.5.3 Pathogenesis
Scarlet fever is a result of infection with group A streptococcus pyogenes infection. Exotoxins A, B and C, also known as streptococcal superantigens , are responsible for causing the cutaneous eruption, strawberry tongue, and skin desquamation [18, 19]. These superantigens stimulate T lymphocytes with ensuing release of massive amounts of cytokines, including interleukin-1 and tumor necrosis factor-α [1, 19].
11.6 Cellulitis
11.6.1 Clinical Features
Cellulitis is defined as “a diffuse and spreading infection with inflammation of the deeper dermis and subcutaneous fat” [20]. Clinically, it is characterized by rapid development of swelling, redness, warmth, and tenderness of soft tissues. Vesicles, bullae, ecchymoses, and petechiae can sometimes be seen. Although certain risk factors, such as obesity and chronic edema, may predispose some patients to recurrences, the overall prognosis is favorable with appropriate systemic antibiotic therapy.
11.6.2 Histology
The histologic findings in cellulitis may be somewhat subtle and nonspecific, and they can vary with the duration of the lesion biopsied. Acute lesions show a diffuse dermal infiltrate of neutrophils and interstitial edema separating dermal collagen bundles. Dermal edema may result in the formation of bullae. In most cases, the inflammatory infiltrate is only moderately intense without frank abscess formation. Blood vessels are dilated, and in some cases they may appear preferentially inflamed. However, there is no actual vasculitis. In resolving lesions, granulation tissue and even fibrosis may be present. Tissue culture may be helpful in identifying the causative bacterial pathogen and antibiotic sensitivity.
The histologic differential diagnosis includes neutrophilic dermatoses such as Sweet’s syndrome that can be easily differentiated based upon clinical presentation. Leukocytoclastic vasculitis may also enter the differential diagnosis, but there is no destruction of blood vessel walls in cellulitis. Erysipelas has identical histologic findings, and is separated purely based upon clinical findings. Erythema marginatum may also demonstrate a diffuse neutrophilic dermal infiltrate without significant vascular damage, but it has a markedly different clinical presentation and is associated with rheumatic fever, which is not a feature of cellulitis.
11.7 Furuncle and Carbuncle
11.7.1 Clinical Features
A furuncle is a deep infection of the hair follicle that forms an abscess [23]. Multiple adjacent infected follicles can sometimes coalesce to form a carbuncle. Furuncles appear as painful red nodules on hair-bearing areas. They may or may not be fluctuant, or have an overlying central pustule. Although some patients develop recurrent episodes, most have a favorable prognosis with appropriate therapy for acute episodes and measures to decrease Staphylococcus aureus colonization of the skin and mucous membranes.
11.7.2 Histology
Histologically, carbuncles and furuncles differ in the location of the inflammatory process within the skin. Furuncles represent dermal abscesses, almost always follicularly centered, that result in destruction of the epithelium and formation of sinus tracts deep within the dermis and subcutaneous fat. Large aggregates of neutrophils are present within the follicular epithelium and diffusely throughout the dermis. A granulomatous reaction is sometimes seen in the regions of follicular destruction. Older lesions demonstrate marked fibrosis and scarring. It is not uncommon to see overlying neutrophilic abscesses, and serum and neutrophil crust.
Carbuncles are larger and more deeply situated abscesses, again with collections of abundant neutrophils. These frequently develop as a result of adjacent furuncles fusing together to form a larger area of inflammation, necrosis, and tissue destruction. These are most commonly seen in the deep reticular dermis and centered within the subcutaneous fat.
11.7.3 Pathogenesis
Staphylococcus aureus is the microorganism most commonly associated with the formation of carbuncles and furuncles [23, 24]. In the majority of cases, these lesions arise from folliculitis that worsens. Patients with underlying systemic illness, such as diabetes, kidney and liver disease, are at increased risk for developing furuncles and carbuncles. Rarely, other bacteria have given rise to these types of lesions [25]. Furuncles may rarely be seen in parasitic conditions, including myiasis [26].
11.8 Ecthyma Gangrenosum
11.8.1 Clinical Features
Ecthyma gangrenosum is frequently a skin manifestation of severe systemic infection, typically with Pseudomonas aeruginosa. Although it is usually seen in neutropenic and immunocompromised patients, it has also been reported in previously healthy individuals [27].
Clinically, lesions often start as erythematous macules, papules, or nodules that develop into hemorrhagic vesicles and bullae, and later progress to necrotic ulcerations with black eschars and surrounding erythema (Fig. 11.6). Lesions usually affect the perineal and gluteal areas (57 %) and the extremities (30 %) [28]. Mortality rate may be as high as 96 % for septicemic cases, but it is reported at 15 % for non-septicemic cases [27].

Fig. 11.6
Ecthyma gangrenosum presents as an ulcerated plaque with rim of erythema at the dorsum of the foot with similar satellite lesions on the toes in an immunosuppressed toddler
11.8.2 Histology
Histologic sections demonstrate skin with marked vascular destruction and thrombosis, often associated with relatively scant inflammatory infiltrate and readily apparent bacterial overgrowth (Fig. 11.7). Blood vessels are necrotic, and there is marked edema and hemorrhage (Fig. 11.8). Gram stains demonstrate abundant gram-negative rods, which can be seen on routine H&E sections as well. In most cases, Pseudomonas aeruginosa is the offending microorganism, but many other microorganisms have been implicated in cases with similar histologic changes.
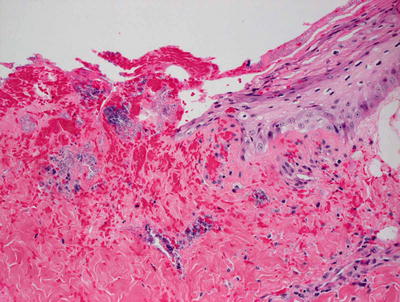
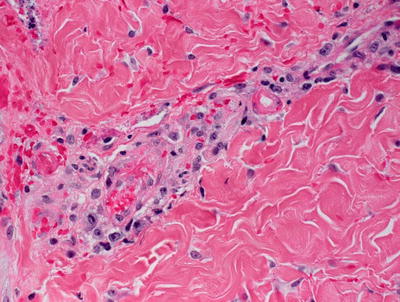
Fig. 11.7
Ulceration and hemorrhage are common findings in ecthyma gangrenosum. Numerous microorganisms are observed on H&E stained sections
Fig. 11.8
Ecthyma gangrenosum demonstrates blood vessels occluded by fibrin thrombi with surrounding hemorrhage
The differential diagnosis includes leukocytoclastic vasculitis, which usually has more neutrophilic infiltrate and less thrombosis. Microorganisms are not seen in leukocytoclastic vasculitis in the absence of septicemia. An invasive fungal process could also demonstrate similar histologic changes, but it can be readily distinguished on PAS stain that demonstrates fungal microorganisms within vascular walls.
11.8.3 Pathogenesis
While most commonly associated with Pseudomonas aeruginosa, bacteria including Escherichia coli, Citrobacter freundii, Klebsiella pneumonia, Staphylococcus aureus, and other Pseudomonas species are also found in ecthyma gangrenosum [29–31]. Rare cases have been associated with Candida albicans and Fusarium infections [31]. Most affected individuals are immunocompromised [29, 30]. Underlying neutropenia and other types of impaired immunity are frequently a contributing cause to the disease, although ecthyma gangrenosum has been seen in patients with normal neutrophil counts [30]. Septicemia is present in some patients with ecthyma gangrenosum [32].
11.9 Erysipelas
11.9.1 Clinical Features
Erysipelas is an acute superficial cutaneous cellulitis, affecting the epidermis and upper dermis. Incidence has been estimated at 10–100 cases per 100,000 individuals per year [33]. It more commonly affects the elderly and small children, as well as those who are immunocompromised. Erysipelas tends to favor the face and legs, although it can occur at other cutaneous sites. It is usually caused by group A β-hemolytic streptococcus.
An erythematous patch that rapidly enlarges, becoming tender, edematous, and indurated characterizes this infectious process . Lesions have well-defined raised borders. With more severe infections, bullae may form, and necrosis can develop. Although some patients with impaired circulation may be at risk for recurrences, those who receive appropriate therapy in a timely manner have an excellent prognosis.
11.9.2 Histology
The histologic findings and differential diagnosis of erysipelas are identical to those seen in cellulitis (Sect. 11.6).
11.9.3 Pathogenesis
Streptococcus pyogenes is the usual cause of erysipelas. However, groups B, C and G streptococci can cause a similar eruption, as can Staphylococcus aureus [34].
11.10 Necrotizing Fasciitis
11.10.1 Clinical Features
Necrotizing fasciitis is a rare severe soft tissue infection. The annual incidence of necrotizing fasciitis in the United States is approximately 500–1000 cases. Although it can affect any age group, it is somewhat more common in patients over the age of 50. The male to female ratio is 3:1 [35]. Typical sites include the extremities, perineum, genitalia, and abdomen . In the early stages of disease, the clinical findings are similar to those seen in cellulitis. There is tenderness, erythema, and swelling of the affected tissues. Pain often becomes severe, and classically appears out of proportion to the physical findings. As the infection progresses, bullae, ecchymoses, and necrosis can develop. Early diagnosis and treatment is critical for a favorable outcome. Even with optimal treatment, disease morbidity is significant, and mortality rates are between 25 and 35 % [36].
11.10.2 Histology
The histologic changes are those of a suppurative process involving primarily the deep subcutaneous fat and underlying fascia (Figs. 11.9 and 11.10). In some cases, the process extends into the deeper portions of the reticular dermis. There is marked vascular necrosis and thrombosis as well as extensive tissue necrosis. Sheets of bacteria are seen on routine H&E stains, and generally not requiring Gram stains in order to be observed. While group A streptococcal infections are implicated in most cases, a wide range of bacteria may cause this process.
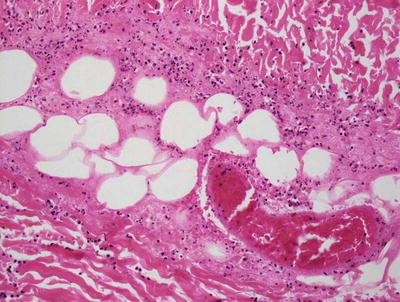
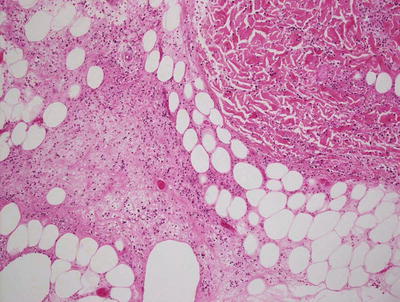
Fig. 11.9
Vascular occlusion by fibrin thrombi, inflammation, and surrounding necrosis of the deep dermis, subcutis, and underlying fascia are seen in necrotizing fasciitis
Fig. 11.10
Total necrosis of the subcutis and a dense neutrophilic inflammatory infiltrate characterize necrotizing fasciitis
11.10.3 Pathogenesis
Necrotizing fasciitis occurs as a result of bacterial infection. While many microorganisms have been implicated, group A Streptococcus pyogenes is the most commonly associated agent. In many patients, there are associated comorbidities, such as diabetes mellitus, which appear to increase the risk for this potentially lethal infectious process [37]. Streptolysin S produced by group A streptococci may play a role in the virulence of this process by attacking keratinocytes and initiating programmed cell death . Furthermore, this toxin incites inflammatory cascades that result in the downregulation of Akt pathway-mediated cytoprotection. Streptolysin S may play a role in facilitating the deep invasion and extensive cellular destruction seen in necrotizing fasciitis [38].
Serotype M3 group A streptococcus is one of the three most frequently associated strains. It has been shown that M3 serotype has a significant ability to evade neutrophil- and TNF-α-mediated responses to infection, resulting in increased microbial ability to invade soft tissue [39]. Group A streptococci also produce SpeB, which is a potent cysteine protease that appears to play a significant role in the virulence of this process [40].
11.11 Meningococcemia
11.11.1 Clinical Features
Invasive meningococcal disease includes meningitis and meningococcemia. Although meningitis is more common (30–60 % of meningococcal cases), meningococcemia accounts for the initial presentation in 20–30 % of cases [41].
A widespread morbilliform blanching rash is often present early in the disease course, and persists in up to 13 % of cases. A petechial and purpuric eruption develops in up to 80 % of patients. In severe cases with disseminated intravascular coagulation, purpura fulminans may develop, often leading to extensive necrosis and loss of tissues. The mortality rate of meningococcemia in developed countries is estimated at 10–20 %.
11.11.2 Histology
Histologic findings are those of a marked vascular occlusive process. Within the dermis, there is widespread thrombosis within blood vessel walls with a mild to moderately intense neutrophilic infiltrate surrounding the vessels (Figs. 11.11 and 11.12). Edema and hemorrhage are seen in most cases [42]. Microorganisms are not ordinarily apparent on H&E sections, although they can be seen on tissue Gram stains, and will be evident with tissue microbiological culture.
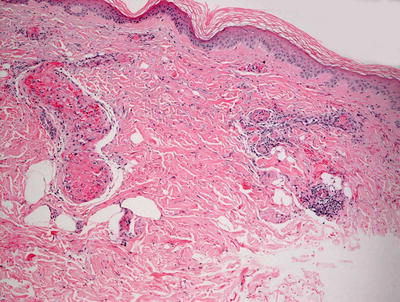
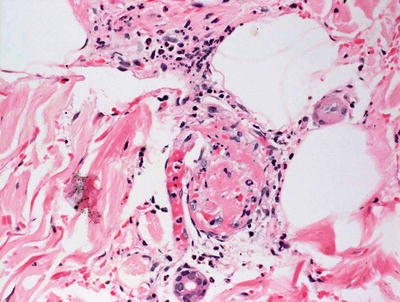
Fig. 11.11
Acute meningococcemia is characterized by distended and thrombosed dermal blood vessels, often lacking significant surrounding inflammatory infiltrate
Fig. 11.12
Fibrin thrombi occlude dermal blood vessels in meningococcemia
The differential diagnosis includes other causes of vascular occlusive disease, including gonococcemia, lupus anti-coagulant, protein C deficiency, and other primary coagulopathies and cryoglobulinemias. Leukocytoclastic vasculitis generally has more inflammation and less thrombosis than is seen with meningococcemia, although other types of septicemia-induced vasculitis may show identical changes. In these cases, tissue microbiological cultures are required to isolate the offending organisms. Henoch–Schonlein purpura can be differentiated based upon the presence of peri-vascular IgA, which is not seen in meningococcemia, as well as by the different clinical presentation [43].
11.11.3 Pathogenesis
Neisseria meningitidis is the causative microorganism of meningococcemia. It is able to invade vascular endothelial cells by remodeling endothelial barriers [44]. Using type IV pili, the microorganism interacts with endothelial cells, resulting in vascular leakage and thrombosis [45, 46]. Furthermore, Neisseria meningitidis produces an endotoxin that results in cytokine-mediated dysregulation of the anticoagulant and procoagulant balance [42]. Interleukin-12, interferon-γ, tumor necrosis factor-α, and interleukin-1 activities can cause a consumptive coagulopathy of proteins C and S, leading to the clinical presentation [42].
11.12 Gonococcemia
11.12.1 Clinical Features
Gonococcemia results from systemic dissemination of untreated primary infection with Neisseria gonorrhoeae. Disseminated infection occurs in approximately 1–3 % of individuals with gonorrhea [47]. Approximately 60 % of patients with gonococcemia develop cutaneous involvement [48]. Typically, skin lesions are few in number and localized to the extremities. They usually begin as small papules that evolve into hemorrhagic pustules. Occasionally, bullae, petechiae, or necrotic areas develop.
11.12.2 Histology
The histologic changes in gonococcemia are identical to those seen in meningococcemia as described in Sect. 11.11 above.
11.13 Erythrasma
11.13.1 Clinical Features
Erythrasma is a skin disorder caused by infection with Corynebacterium minutissimum. It is more common in patients who are overweight, elderly, and diabetic, especially in warm climates [49]. It tends to occur in intertriginous areas, such as the inguinal, interdigital, intergluteal, and inframammary creases.
Clinically, lesions appear as well-defined red brown patches and thin plaques. Mild pruritus may be present, although most cases are asymptomatic. Examination with a Wood’s lamp shows bright purple red fluorescence of affected areas. With appropriate therapy , the prognosis is excellent, although some patients may be prone to recurrences. Immunocompromised patients may sometimes progress to serious systemic infections.
11.13.2 Histology
Biopsies are rarely performed when a diagnosis of erythrasma is clinically suspected. Clinical diagnosis is usually confirmed with Wood’s light examination. Histologic changes in skin biopsies are quite subtle. Within the stratum corneum, small foci of parakeratosis are present within which microorganisms may be identified (Fig. 11.13). The term “Chinese characters” has been given to the angulated Corynebacteria that are usually evident with routine H&E staining, but they can be highlighted with tissue Gram stains. Minimal epidermal spongiosis may be present, and there is usually a scant lymphocytic inflammatory response.
Fig. 11.13
Subtle histologic findings in erythrasma are limited to small foci of bacteria within the stratum corneum with virtually minimal inflammation
The main histologic differential diagnosis is that of normal skin. Close examination of the stratum corneum and clinical correlation will lead to an accurate diagnosis in most cases. While dermatophytosis may have similar histologic changes, PAS stains clearly make the distinction. Candidiasis is usually more inflammatory with abundant neutrophils within the epidermis and occasionally within the superficial dermis.
11.13.3 Pathogenesis
Erythrasma is the direct result of colonization by Corynebacterium minutissimum. There is some ultrastructural evidence that suggests the microorganisms are able to invade the stratum corneum by inducing keratolysis [50].
11.14 Malakoplakia
11.14.1 Clinical Features
Cutaneous manifestations are quite unusual in malakoplakia. When present, they most often occur in the genitourinary skin, although lesions have been described in other sites. Lesions are soft, yellow friable plaques and nodules. Malakoplakia is more common in immunocompromised individuals [51, 52]. Treatment with antibiotics may be helpful in resolving cutaneous lesions [53].
11.14.2 Histology
Malakoplakia rarely involves the skin. However, the histologic changes in the skin resemble those seen in other sites. In malakoplakia, aggregates of foamy macrophages fill the dermis. Granulomatous inflammation is often present surrounding foamy macrophages. These cells are filled with calcified basophilic spherules known as Michaelis–Gutman bodies. The spherules are highlighted on PAS, Perl’s iron, and von Kossa stains [53]. Bacteria are not readily apparent on routine H&E stains, but they can be identified with antibodies directed against mycobacterium bovis [54].
11.14.3 Pathogenesis
Although not fully understood, malakoplakia is widely believed to be the result of an acquired bactericidal defect within macrophages that is frequently encountered in immunosuppressed individuals and those with autoimmune disorders [51, 52]. In malakoplakia, macrophages engulf bacteria appropriately, but their ability to digest the microorganisms intracellularly is impaired [55].
11.15 Tuberculosis
11.15.1 Clinical Features
Cutaneous tuberculosis presents with a wide variety of skin lesions, including papules, verrucous plaques, and chronic ulcers. There are four major categories of cutaneous tuberculosis [56].Cutaneous tuberculosis caused by inoculation from an exogenous source include primary inoculation tuberculosis or chancre, and tuberculosis verrucosa cutis. In primary inoculation tuberculosis, a firm reddish brown papulonodule develops 2–4 weeks after inoculation and slowly enlarges, sometimes resulting in a friable ulcer or verrucous plaque. Tuberculosis verrucosa cutis begins as erythematous papules surrounded by a purple halo, and evolve into asymptomatic verrucous plaques that may ulcerate or develop central atrophy.Cutaneous tuberculosis resulting from endogenous spread, either contiguously or via autoinoculation, include scrofuloderma and orificial tuberculosis. In scrofuloderma, painless, cold abscesses develop and often evolve into plaques with draining fistulae. The most common site is the cervical lymph node chain. In orificial tuberculosis, lesions are friable, erythematous and painful papules and nodules that develop into painful ulcers.Cutaneous tuberculosis resulting from hematogenous spread include lupus vulgaris, acute miliary tuberculosis, and tuberculous gumma, ulcer or abscess. In lupus vulgaris, lesions appear as papules, nodules, or reddish brown plaques. In acute miliary tuberculosis, erythematous papules and vesicles appear, sometimes with overlying crust. In tuberculous gumma, ulcer or abscess, there are a few subcutaneous nodules scattered over the trunk and extremities.Cutaneous tuberculosis associated with an underlying focus of infection (tuberculids) include papulonecrotic tuberculid, lichen scrofulosorum, and erythema induratum (also known as Bazin disease). Papulonecrotic tuberculid presents as an eruption of papules and pustules that affect the face, ears, trunk, buttocks, and extensor extremities. Lichen scrofulosorum is characterized by plaques that are composed of indurated grouped small red papules, most commonly located on the trunk. Erythema induratum is characterized by reddish purple subcutaneous nodules over the posterior thighs and legs of young and middle aged females.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


