Pearl
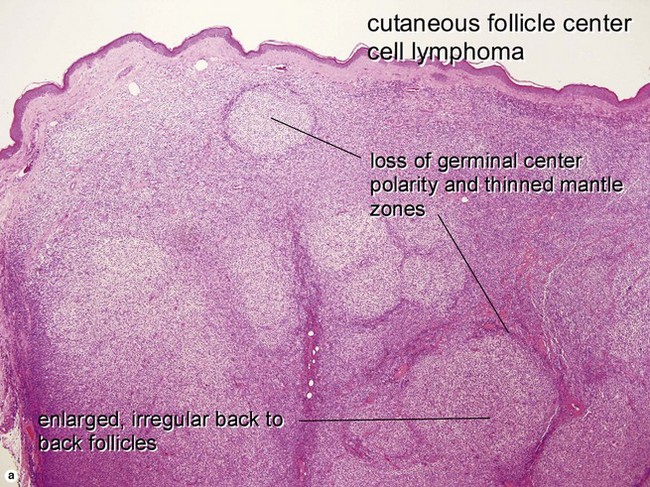
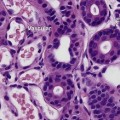
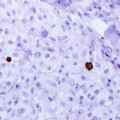
In primary cutaneous follicle center cell lymphoma, the BCL-6-positive cells typically stray outside of the follicle. BCL-2 expression is characteristic of follicle center cell lymphoma in lymph nodes, but is rare in the primary cutaneous variety. At cutaneous sites, BCL-2 positivity in a follicle center cell lymphoma should raise suspicion for a nodal primary with secondary involvement of the skin.