Chapter 22 Autoimmune connective tissue diseases
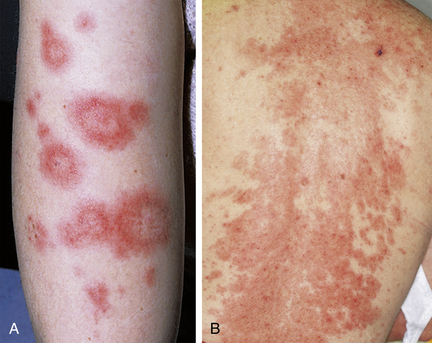
Lupus patients also develop many skin changes that are not specific for LE, termed lupus-nonspecific eruptions (Table 22-1). These eruptions do not help to establish a diagnosis of LE, but they may still be very important to note, as specific systemic findings may be associated with them. For example, cutaneous lesions of palpable purpura in a patient with LE are not lupus-specific, that is, such lesions may be seen in patients who do not have LE; however, they may be associated with vasculitic lesions of the kidney or central nervous system (CNS), and thus they have significance in the evaluation and treatment of lupus.
Table 22-1. Classification of Cutaneous Disease in Lupus Erythematosus
| LUPUS-SPECIFIC ERUPTIONS | LUPUS-NONSPECIFIC ERUPTIONS |
|---|---|
(Discoid lupus erythematosus (DLE), hypertrophic DLE, tumid LE, chilblain LE, lupus mucinotic nodules) |

Figure 22-1. Acute cutaneous lupus erythematosus. Note the classic malar erythema (“butterfly rash”).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


