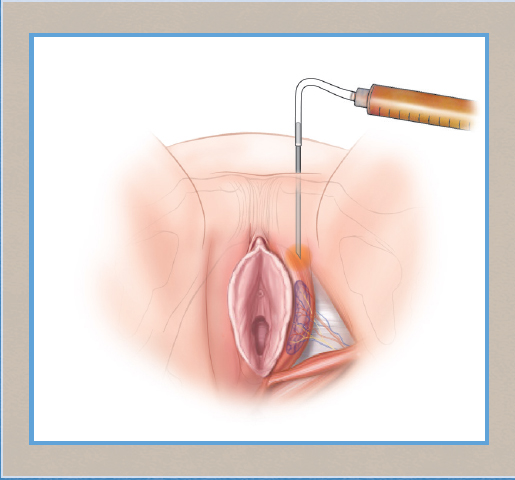
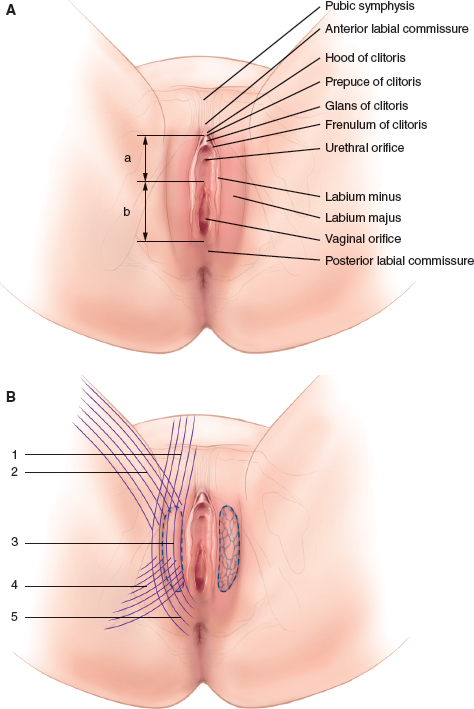
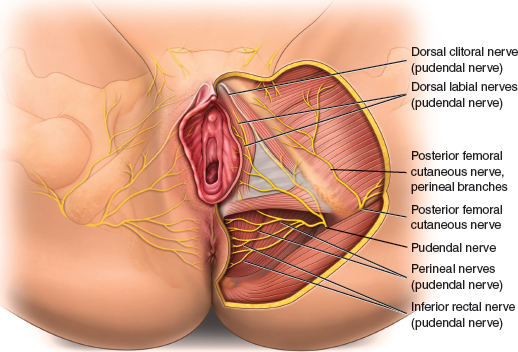
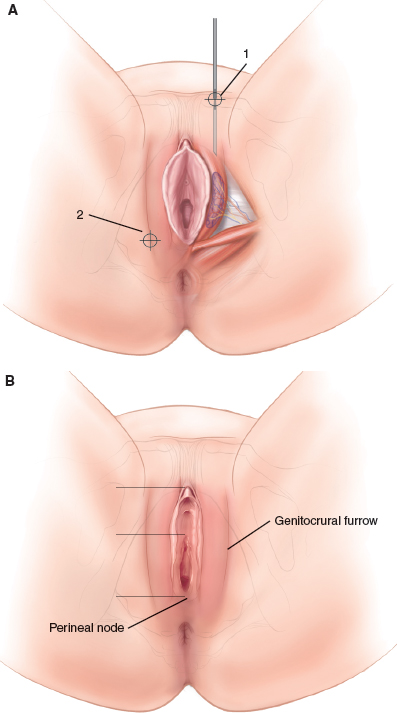
CHAPTER 9 • The use of specific injectable hyaluronic acids (HAs) for the reconstruction and remodeling of the labia majora provides an effective, reversible, and safe treatment that is dependent on surgeons’ excellent anatomic and functional knowledge of the genital area, their mastery of the technique, and the quality of the products used. • Rejuvenation or restoration of the vulvovaginal region with heterogeneous biodegradable products such as HA promises to be an area of extensive development, especially in synergy with other current or future nonsurgical methods. The labia majora play a vital role in protecting the labia minora (nymphs) in the superior part of the vestibule and the introitus (lower third of the vagina) in the posterior part. This protection prevents unwanted friction of the labia minora, particularly friction pain from sports activities (for example, horseback riding and bicycling) or tight and form-fitting clothes. Hypotrophy of the labia majora is a cause of chronic vulvitis and vulvovaginal dryness, causing discomfort, pruritus, and intromission dyspareunia. Functional, psychological, and sexual consequences are real limitations in women’s lives and can affect sexuality, libido, and self-confidence. The aesthetic of the vulval area depends on the blending of the mons pubis subcutaneous tissues covering the pubic bone with the upper labia majora. The growing desire of women to correct or retain the youthful appearance of a more sensual genital area was probably amplified by the growing popularity of pubic and vulval hair removal,1 but it also results from the desire to erase the consequences of aging, childbirth, and various injuries. Anatomic understanding of the vulvovaginal region is essential to the practice of genital rejuvenation and restoration techniques. The intricate complexity of the relationship between the superficial and deep structures and the intimate relationships among the skin, mucous membranes, muscles, ligaments, and fascia define these anatomic and functional units.2 The labia majora are formed by a skin surface comprising stratified squamous epithelium (keratinized and pigmented), dense vascular dermis rich in sebaceous glands, apocrine glands, and a deep layer of smooth muscle fibers: the labial dartos (Fig. 9-1). Other components of the labia majora include a fatty layer under the skin that regresses with aging or excessive weight loss and a labial fat corpus, which is both a fibrofatty formation rich in vessels and a semierectile organ reinforced by elastic fibers with fibrous expansions that push it forward, sideways, and backward. Regression of fatty tissue of the labia results from the gravitational effect of body weight on the perineum and from the repetitive friction movement of the thighs. Fig. 9-1 A, The superficial perineum. B, Dissection of the corpus under the dermis and superficial fat to view the labial fat. (a, Urethral part of vestibule; b, hymenal part of vestibule; 1, puboclitoris conjunctive expansion; 2, inguinal expansion; 3, labial adipose corpus; 4, gluteal expansion; 5, perineal expansion.) During aging, the skin surface of the labia undergoes the same degradation as the body’s dermis. The labia majora fatty subcutaneous plane undergoes a “fat melting” or lipoatrophy. This creates a deflated appearance and hypotonicity, with volume loss of the filling material and a wrinkled appearance of the skin surface. This loss of protection also affects the labia minora and vestibule, which results in vulvovaginal dryness, spontaneous or induced pain during sexual intercourse, and compensatory hypertrophy of the labia minora by sliding of the dermis.3 Hypotonia associated with subcutaneous lipoatrophy causes the dermis overlying the labia majora to relax and extend into the dermis of the outer face of the labia minora, increasing their relief. The main principles of the remodeling or restoration of the labia majora are based on reconstruction of the different planes: • Superficial labia majora dermal rejuvenation is similar to the rejuvenation and biorevitalization of the dermis of the face: – Non-cross-linked or weakly cross-linked HA injected intradermally or superficially by needle, roller, microneedle, or injector gun according to well-known techniques in mesotherapy – The use of platelet-rich plasma in multiple injections, alone or combined with HA, which allows a remarkable reconstruction of the thickness of the dermis, eliminating vulval wrinkles, fine lines, and folds. • Deep dermal labia majora rejuvenation treatments improve the tone of the labial and vulval muscles (dartos), the trophicity, and the youthful appearance of the labia majora. Radiofrequency techniques and thermal effects applied to the genital area remarkably correct vulvovaginal loss from aging or trauma of childbirth through its effects on neocollagenesis and smooth muscle tone (see Chapter 16). • In continuity with the fatty tissue of the pubic region, the fatty tissue of the labia helps to enhance the relief of the labia majora and distinguish between the hairy external side and the glabrous inner side. This subcutaneous fat is made up of a superficial layer and a deep level that covers the surface area of the perineum. The Bartholin glands and erectile bodies, with their various muscles and fascias, are located between the superficial fascia of the perineum and the perineal membrane (or the lower fascia of the urogenital diaphragm), which comes in contact with the deep layers of fatty tissue. Bulbospongiosus muscles cover the vestibular bulbs, and ischiocavernosus muscles overlie the corpora cavernosa3 (Fig. 9-2). The loss of thickness of the fatty tissue associated with causes such as aging (after menopause), estrogen loss, significant weight loss (postpartum weight loss), and everyday microtrauma (from sports, tight clothes, hair removal) can accelerate skin aging. This results in a general “loosening” with collapse of the vulval relief skin and deep wrinkles. The outline of the labia majora—with an outer surface, an inner surface, and a protruding free edge—is created by the same subcutaneous fatty tissue. It gives the appearance of an inverted V. Fig. 9-2 The superficial perineal fascia and perineal membrane. Correcting this fatty atrophy by injections of HA is an alternative to lipofilling. This nonsurgical, minimally invasive genital rejuvenation method is particularly attractive for its simplicity of implementation, its in-office practice facility, and its convincing results. • Women older than 18 years of age • Patients who desire aesthetic rejuvenation of the labia majora or to protect the vulva and the labia minora • Male sex • Pregnant or breast-feeding women • Known hypersensitivity to one of the injected components (for example, HA and mannitol) • Vulvovaginal infections in the injection site (bacterial, viral such as herpes or HPV, or fungal) • Skin problems like inflammation near the injection area • The presence of semipermanent or permanent products in the area to be treated • Recent vulval surgery in the treatment area or progressive recent or nearby cancers • A history of autoimmune disease, streptococcus disease, or acute rheumatic fever with cardiac localization The assessment of lipoatrophic labia majora, and therefore the amount needed to be injected, is made by comparing and assessing the thickness of the pubic fat and the protrusion of the labia minora. We need to find an aesthetic and functional balance between these structures. Patients are given 3 days’ antiseptic treatment with intravaginal ovules of neomycin with polymyxin B and nystatin. During the 3 days before the intervention, no hair is removed from the vulva by shaving or any other means. We ask patients with significant vulval hair growth to perform a “deburring” 2 or 3 days before the procedure. This involves cutting the hair with scissors to a length of 1 cm. Before the injection, a careful surgical antiseptic prep is performed, with at least three passes throughout the dermal surface, the vulva, and intravaginally. (We usually use povidone iodine 10%, occasionally, chlorhexidine gluconate or benzalkonium chloride.) Xylocaine 2% is injected intradermally, 0.2 ml on each side. These injection sites will be used again. We also inject deeply and subcutaneously (five to seven injections of 0.3 ml) along the future path of the cannula, following the line previously drawn, described below. Several points of introduction are possible, depending on the position and preference of the operator. Fig. 9-3 shows points that are safer and more consistent with anatomic characteristics. The upper points I use are in the lateropubic area, two to three finger-breadths on each side of a vertical center line, between the pubis and the posterior commissure. The lower points and the points 2 cm lateral to the labia minora constitute the posterior commissure. For these injections, the patient is in a lithotomy position, and the surgeon inserts the needle or the injection cannula upward and diagonally toward the genitocrural furrow.
Augmentation of the Labia Majora With Fillers
Nicolas Berreni
Key Points
Anatomy and Histology
Indications and Contraindications
Indications
Contraindications
Contraindications Related to Hyaluronic Acid
Patient Evaluation
Preoperative Planning and Preparation
Surgical Technique
Anesthesia
Markings
Related posts:
 Fractional Erbium Laser for Vaginal Rejuvenation
Fractional Erbium Laser for Vaginal Rejuvenation
 Labia Majora Reduction Surgery: Majoraplasty
Labia Majora Reduction Surgery: Majoraplasty
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
 Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
 Augmentation of the Labia Majora With Fat Grafting
Augmentation of the Labia Majora With Fat Grafting
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine
