Chapter 6 Augmentation Mastopexy
Introduction
For many patients, breast hypoplasia and ptosis of either the gland or the nipple–areola complex (NAC) very often occur together. Perhaps the most common scenario for this presentation is the postpartum patient who presents after having delivered and breast-fed several children. After the transient increase in breast size that stretches out the supporting structures of the breast, involution may occur that then leaves the skin envelope variably underfilled and ptotic. Also, the NAC is very often positioned low on the breast mound (Figure 6.1). In these patients, simply performing a breast augmentation alone can result in a superiorly malpositioned implant in relation to the breast mound and an NAC position that remains far too low to be aesthetically acceptable (Figure 6.2 A,B). Conversely, performing a mastopexy alone may leave the remaining breast skin envelope underfilled as there is often not enough existing breast parenchyma to provide the result the patient is trying to achieve. For these reasons, to obtain the best result, it becomes necessary to combine the two procedures. While the rewards for such a surgical undertaking can be tremendously gratifying, the difficulty of the procedure is greater than for either operation alone. This is related to the fact that the two operations have opposing goals. Breast augmentation increases the volume of the breast and therefore expands the surface area to accommodate the new volume. In contrast, mastopexy generally reduces the skin surface area in the process of accomplishing the lifting of the NAC. Therefore, any operative procedure designed to treat hypoplasia with ptosis must artistically coordinate these two competing surgical maneuvers in such a manner so as to allow a lifting of the NAC and a reduction in the skin envelope but yet leave behind enough skin to easily accommodate the new breast volume provided by the implant. Also, these goals must be accomplished in a manner that reliably preserves the blood supply to the NAC, results in the least amount of cutaneous scar possible and provides an aesthetic and long-lasting result, all in one operation. When viewed in this context, it is easy to understand why many surgeons believe augmentation mastopexy to be one of the most challenging aesthetic procedures performed on the breast. However, by strategically applying the principles outlined in the previous chapters on augmentation and mastopexy, a sound and reliable surgical plan can be developed that will allow these two procedures to be combined successfully.



Indications
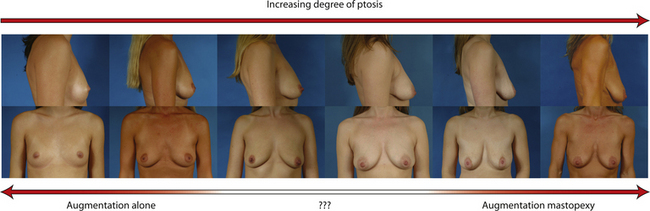
In evaluating patients for breast augmentation, it is easy to recognize those patients who have an NAC position that is located well up onto the breast and who will do well with the simple placement of an implant. In these patients, the NAC will end up being located directly at the apex of the breast and an aesthetic relationship between the breast mound and the NAC position can be achieved. Conversely, it is also easy to identify those patients who have such profound ptosis that nothing short of a mastopexy will restore balance to the breast mound and nipple position. However, there are many patients who present for breast augmentation who seem to fall in between these two extremes (Figure 6.3). Not only is the breast deficient in volume, but the location of the NAC falls somewhere between the apex of the breast and the lower breast border. This anatomic relationship is extremely common, particularly in postpartum patients, and it presents for the plastic surgeon one of the most difficult decisions that must be made in the patient with breast hypoplasia, namely, when to add a mastopexy to the overall operative plan to achieve the best result. The difficulty in making this decision lies in the fact that ptosis is not an all or none phenomenon. How much ptosis in the position of the NAC that can be accepted and still have a reasonable result may well come down to a matter of personal preference for both the patient and the surgeon. Whether to accept a slightly less than ideal breast volume to NAC relationship must be weighed against the scar that would be created on the breast to accomplish the mastopexy. Many patients are reluctant to accept anything more than an inconspicuous inframammary fold or transaxillary scar and will therefore accept a slightly low NAC position to avoid an additional scar on the breast. However, determining exactly where the NAC will end up in relation to the remainder of the breast can be difficult as the simple act of adding an implant to the underfilled skin envelope of the breast will result in a minor lifting effect on the NAC and how much lift will be achieved can be difficult to predict. One preoperative anatomic relationship I have found useful in making the decision of whether or not to perform a mastopexy with the augmentation involves observing the position of the nipple in relation to the inframammary fold (IMF). This relationship is assessed by drawing a line across the chest connecting the most inferior extent of the two inframammary folds together and then standing back and observing where the nipple lies in relation to this fold line (Figure 6.4). In the case of a fold asymmetry, it is advisable to base decisions on the higher of the two folds as this will be the rate-limiting contour influencing the final result. By using this static line drawn across the midline, an accurate determination of where the nipple lies in relation to the fold can be made without to need to perform any lifting or other manipulation of the breast. Assuming the location of the IMF remains unchanged and stable postoperatively, it is then possible to use the nipple to fold relationship as a guide to assessing the need for a mastopexy. Three types of relationships are possible:

Nipple above fold – This is the easiest clinical presentation to manage as the vast majority of patients will achieve an aesthetic result with simply an augmentation alone. Of course, the higher the position of the NAC the better, as the ideal location for the NAC after the placement of the implant is at the most projecting portion of the new breast mound. However, even in patients where the nipple is just slightly above the fold, a reasonable result can be obtained using standard augmentation techniques and incision locations without the need for a mastopexy (Figure 6.5 A–G). One nuance that can be utilized in these types of patients is to lean more towards a periareolar approach for the breast augmentation rather than using an inframammary or transaxillary incision. In this fashion, should a periareolar mastopexy ever become necessary in the future, the extra scar burden is minimized since half the scar is already present.







One unique clinical situation where a mastopexy is indicated despite the fact that the nipple is above the fold involves the occasional patient who presents with pseudoptosis. In these cases, a significant portion of the gland can descend into the lower pole of the breast and yet the NAC is positioned normally. Typically, the skin envelope in the lower pole is redundant and underfilled. This clinical presentation is potentially troublesome and must be recognized preoperatively as simply inserting an implant in this type of patient can create an over-expansion of the lower pole and result in an exaggerated and overly rounded lower pole contour with an NAC position which appears to be superiorly displaced. Therefore, while these patients do not necessarily require a periareolar mastopexy, they can often benefit from a ‘vertical’ mastopexy where the redundant and ptotic skin and gland of the lower pole of the breast is plicated from the bottom of the areola down to the IMF to create the desired lower pole shape. By taking up the excess tissue in the lower pole of the breast, the position and shape of the breast mound are brought into better harmony with the position of the NAC. Also, the vertical incision affords ready access to the breast and can easily be used to develop the pocket and place the implant. This very straightforward and easily performed technique adds a powerful shaping strategy to the overall operative plan and can lead to excellent results in appropriately selected patients (Figure 6.6 A–G).






Nipple at the fold – Many patients present with one or both nipples at or very near the level of the inframammary fold. It is in these patients that the decision to perform a mastopexy becomes difficult. Both the patient and the surgeon are eager to avoid placing any more scars on the breast than are absolutely necessary and this leads to an understandable reluctance on the part of both to proceed with mastopexy. One surgical maneuver that can be used in these types of patients is to lower the inframammary fold as part of the surgical approach. Although this can result in an overall breast contour that appears somewhat low on the chest wall, the volume provided by the breast implant ends up being properly positioned directly under the NAC. Therefore, as far as the location of both the NAC and the breast mound is concerned, the breast implant is aesthetically positioned. If the degree of lowering of the overall breast position is not excessive, this approach can be used to great advantage. In these cases, it is helpful to use an anatomically shaped gel implant to avoid a contour irregularity in the upper pole of the breast. The more natural upper pole slope of these types of devices helps prevent an unaesthetic step off from becoming visible as could occur with, for instance, a round saline device. Also, because the volume of a shaped cohesive gel implant is more aggressively distributed in the lower pole of the device, there is a more effective filling out of the lower pole of the breast, which tends to lift the NAC position to greater extent than a round implant does (Figure 6.7 A–F). In essence, this strategy involves lowering the implant to fit the breast, which stands in contrast to the usual augmentation mastopexy strategy, which involves raising the breast and NAC to fit the implant. Not all patients are candidates for this approach as there is a limit as to how far the fold can be lowered without creating significant shape or breast position problems. For this reason, many patients who present with the nipple at the level of the fold benefit from the inclusion of a mastopexy done in conjunction with the breast augmentation.






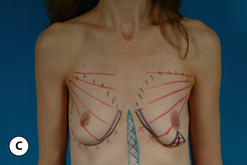
When the nipple is located at the level of the fold and the decision has been made to incorporate a mastopexy with the breast augmentation, this can most often be accomplished with a periareolar approach alone. It can be rationalized that the resulting periareolar scar is only slightly more extensive than would be associated with a traditional periareolar incision alone for breast augmentation where the scar is limited to the lower half of the areolar border, and the improvement in the overall aesthetic appearance of the breast seems worth the extra scar burden. However, the major drawback to the periareolar approach remains the flattened breast contour that can result when the dimensions of the periareolar pattern become too large. Not only does the apex of the breast appear flattened, but the contour of the lower pole appears to bulge, which creates an overly rounded appearance. In selected cases, this bulging can be partially corrected by extending the lower portion of the periareolar pattern slightly inferiorly into the lower pole breast skin. By taking up this redundant skin into the periareolar pattern and combining it with a breast augmentation, the excess lower pole skin is reduced and it may be possible to avoid placing a vertical scar on the breast to correct this contour deformity. However, there is a limit to which this maneuver can be applied without creating a periareolar defect that is too large to be comfortably managed and, if the overall shape of the breast appears distorted or flattened in any way, it may become necessary to add a vertical component to the skin pattern. Typically, depending on the other variables involved for a particular patient, the NAC can be lifted up to 6 cm using a periareolar pattern alone without creating a significant deformity (Figure 6.8 A–C). Beyond 6 cm, a circumvertical skin pattern becomes increasingly necessary to appropriately take up the redundant skin envelope, particularly in the lower pole, and restore an aesthetic breast contour. This is a decision which is easily made at the time of surgery. After placement of the implant, the proposed periareolar pattern can be plicated into position to assess the breast contour. The effect of adding a vertical component can then be assessed. Typically, if the contour of the breast is improved even slightly by adding the vertical component, it is advisable to incorporate this into the pattern. Most patients will be more satisfied with an aesthetic breast contour with a vertical scar than a flatted and distorted result with only a periareolar scar. With adequate preoperative education, most patients can accept the vertical scar as a necessary part of their procedure.








Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


