Augmentation rhinoplasty is one of the most frequently performed cosmetic surgeries in Asia. Because of the United States’ increasing Asian populations, Asian rhinoplasty also has become a common procedure in many larger American cities. As the frequency of Asian rhinoplasties performed increases, so does the demand for revision surgeries on Asian patients who have developed complications or who are unhappy with previous results. This chapter will first review the unique anatomical differences between Asian and Caucasian noses. It will then discuss various possible reasons for revision surgery, as well as medical and surgical treatment options.
 Goals of Asian Rhinoplasty
Goals of Asian Rhinoplasty
Compared with Caucasian noses, Asian noses typically have (1) a lower bony and cartilaginous dorsum, (2) weaker and smaller lower lateral cartilages, (3) thinner, shorter septal cartilage, and (4) thicker skin and subcutaneous tissue.1 Because of these anatomical differences, Asian patients seeking cosmetic surgery often demand higher nasal dorsums, more projected and defined tips, and narrower alar bases.
 Use of Implants
Use of Implants
To achieve higher dorsum and tip projection, various alloplastic implants have been widely used in Asian patients for decades. These alloplastic implant materials include ivory, silicone elastomer, hydroxyapatie, proplast, Medpor (Porex Surgical Inc., Newnan, GA), and Gore-Tex (W. L. Gore & Associates, Inc., Flagstaff, AZ). Of these, silicone elastomer has been the most frequently used material, although Gore-Tex has become increasingly popular in recent years. Other options include autogenous grafts such as calvarial or iliac bone grafts, auricular cartilage grafts, and costal cartilage grafts.
Silicone implants are inexpensive, easy to carve, and easily removed during revision rhinoplasty; for this reason, they are often used in Asian rhinoplasty (Fig. 14–1). They are also well tolerated. In one surgeon’s 10-year experience,2 with 98% of the study population being Southeast Asian, only 0.5% of patients in the 422-patient series required implant removal because of extrusion. There were no removals of implants because of infection. However, these grafts frequently result in capsule formation and are heavier, resulting in a high frequency of migration. Indeed, in the previously mentioned study,2 5.5% of patients required removal of the implant within the first 30 days because of displacement, excessive prominence, hemorrhage, or excessive pressure in addition to obvious supratip deformity; another 4.3% underwent removal after long term follow-up because of displacement or poor aesthetic outcome. In addition, silicone implants are more likely to become distorted from calcification (Fig. 14-2). Another disadvantage is thinning of the overlying skin that gives a glassy, shiny appearance to the dorsum of the nose.
Gore-Tex is another implant in rhinoplasty that has been used with good success (Fig. 14-3). Compared with silicone implants, Gore-Tex implants are less likely to form capsules; they are also less likely to migrate, because they are lighter. However, Gore-Tex is more expensive and difficult to carve intraoperatively than is silicone. In one case series of 309 primary or revision rhinoplasty operations,3 only 3.2% of cases necessitated removal of this kind of implant. All implants were removed secondary to infection, with no report of migration of the implant. Gore-Tex is also technically more difficult to remove in revision cases.
 Challenge of Asian Revision Rhinoplasty
Challenge of Asian Revision Rhinoplasty
Revision rhinoplasty in the Asian population presents a unique challenge to the facial plastic surgeon. The most challenging part of revision rhinoplasty in Asian patients is that the surgeon frequently cannot diagnose underlying problems on the basis of physical examination alone. Many patients seeking revision surgery have had previous operations in another country, and often the operative report of that previous surgery is unavailable. Moreover, it is usually difficult to predict what lies underneath implants and grafts. Here is an example of a patient whose saddle nose deformity was reconstructed with a silicone implant 10 years ago (Fig. 14-4). Should this patient seek revision surgery, the new surgeon would have the challenge of guessing what types of cartilaginous and bony structures exist below the silicone implant.
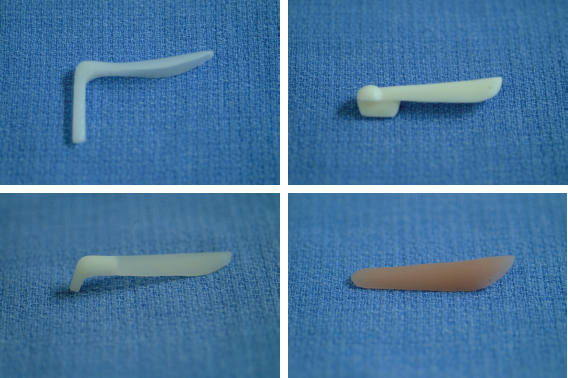
Figure 14–1 Various types of silicone elastomer implants.

Figure 14–2 Calcified silicone implants removed during revision rhinoplasty. (Courtesy of Dr. Dong Hak Jung.)

Figure 14–3 Preformed Gore-Tex implant.
 Specific Problems of Asian Revision Rhinoplasty
Specific Problems of Asian Revision Rhinoplasty
Most Asian revision rhinoplasties are performed as a result of either implant extrusion or infection or unwanted cosmetic results after graft implantation.

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


