2 Blepharoplasty is undoubtedly the most complex aspect of Asian cosmetic surgery, as the eyes are the single most distinguishing feature of the Asian face, and several surgical variations are available. Although most attention, deservedly, has been directed toward upper blepharoplasty, surgery of the lower eyelid is also worthy of special consideration. Upper blepharoplasty is the most commonly requested cosmetic operation by Asian patients, and because of the large Asian population now residing in the West, it is important that aesthetic surgeons have a working knowledge of techniques available for this procedure. Although, strictly speaking, upper blepharoplasty in the Asian is a variation of standard upper blepharoplasty as performed in the Caucasian patient, important anatomic differences that characterize the Asian eyelid warrant intensive description and study of possible surgical options. This is a challenging procedure that requires focused preoperative planning and meticulous attention to intraoperative detail if consistent aesthetic results are to be achieved. One of the major differences between Asian blepharoplasty and standard upper blepharoplasty in the Caucasian is the flexibility in sculpturing upper-eyelid configuration offered by relatively subtle variations in surgical technique. Differences in the level of the palpebral fold and depth of the palpebral sulcus produce substantial effects on the appearance of the eyelid. Aesthetic surgeons who wish to become expert in this operation must possess a clear understanding of the interactions between the various factors that allow construction of upper eyelids that vary in size and shape. The goal of this chapter is to provide more than a basic description of upper blepharoplasty in the Asian patient—a system for reliable construction of an upper lid of a specific size and shape and a system for staged modification of the epicanthal fold are presented. Gone are the days in which a surgeon could perform the same operation on every Asian upper eyelid; the ability to individualize each and every operation is essential to success in the contemporary environment. All surgeons owe their patients an opportunity to choose the type of eyelid transformation that they desire; patients should not be condemned to construction of the classic “westernized” eyelid that was the sine qua non of this procedure in earlier years. The first step in the study of Asian upper blepharoplasty is to understand the Asian colloquialisms “single eyelid” and “double eyelid.” At least 50% of East Asians demonstrate a single eyelid, so termed because in the absence of a superior palpebral fold, the upper lid drapes like a single, unruffled curtain from the supraorbital ridge to the eyelashes (Fig. 2-1). Surgical creation of a palpebral furrow divides the single eyelid into two well-defined segments (pretarsal and preseptal), thus producing the “double eyelid” (Fig. 2-2). Although the popularity of upper blepharoplasty in Asia has undergone a quantum leap since the 1950s, it would be erroneous to assume that this popularity is solely related to Western influences in Asia. Asian cultures have long regarded the alert and bright-eyed look imparted by a double eyelid as aesthetically desirable, and the first surgical description of Asian upper blepharoplasty was published in Japan in the late 19th century. The majority of Asians who have natural “double eyelids” exhibit a rudimentary or small fold associated with abundant periorbital fat and excess eyelid skin. Many of these individuals desire surgical enhancement of this lid configuration, and thus Asian upper blepharoplasty is not restricted to individuals demonstrating “single eyelids.” Figure 2-1 The single eyelid. In the absence of a superior palpebral fold, the lid hangs like an unruffled curtain from the supraorbital ridge. A third facet of Asian upper blepharoplasty is management of the aging lid in individuals who possess natural palpebral furrows or who have previously undergone “double lid” surgery. Prior to proceeding further, it is of paramount importance to emphasize that the aesthetic surgeon must clearly understand that, at the present time, a patient’s request for surgical modification of the eyelid is usually not a request for “westernization “of the eye. In actuality, the vast majority of contemporary Asian patients, particularly those who have been born in Western countries, wish to maintain the character of the upper lid, enhancing its natural beauty. Westernization requires reduction of lid fullness and creation of a large, deep-set upper lid by removing large amounts of skin and fat as well as effacement of the epicanthal fold. In contrast, contemporary Asian upper blepharoplasty is characterized by placement of incisions closer to the ciliary margin, resection of smaller amounts of skin and fat, and conservative manipulation of the epicanthus in patients who request modification of this structure. In my experience, westernization procedures have been requested with markedly decreased frequency during the past 20 years and are sought primarily by recent immigrants to the West. Significantly, patients who have undergone westernization procedures years ago often request surgery to create a more “natural” look that “matches” the Asian face. As such surgery is fraught with difficulty, and the desired results are often impossible to fully achieve, it is incumbent on the surgeon to understand the desires of each patient regarding postsurgical eyelid appearance to avoid patient unhappiness by production of a result that may be difficult or impossible to modify satisfactorily. Figure 2-2 The double eyelid. Creation of a palpebral sulcus divides the lid into two well-defined (pretarsal and preseptal) segments. A commonly accepted anatomic explanation of the difference between the single and double eyelid has formed the basis for Asian upper blepharoplasty in the past: In the double eyelid, filaments of the levator expansion penetrate the orbital septum and orbicularis muscle, attaching to the overlying dermis thus creating a superior palpebral fold when the lid is opened, dividing the upper lid into two distinct segments (Fig. 2-3). In the single eyelid, these levator filaments, rather than penetrating the orbital septum and orbicularis muscle, terminate on the tarsal plate, and thus no palpebral fold is formed upon eyelid opening, the upper lid consisting of a single unit (Fig. 2-4). Although this description has proven to be useful in planning surgical procedures for creation or modification of the palpebral fold, such traditional teaching is an oversimplification. Contemporary anatomic studies have found no evidence of a direct attachment between levator filaments and the dermis, suggesting instead that filaments of the aponeurosis course inferiorly into the pretarsal segment of the eyelid, attaching to fibrous septa that course from tarsus to pretarsal skin (penetrating pretarsal orbicularis), thereby producing adherence between the pretarsal skin, orbicularis, and tarsus. Figure 2-3 Anatomy of the Caucasian (“double eyelid”) upper eyelid. It is the adherence of these tissues that is responsible for creation of the superior palpebral fold, creating a boardlike pretarsal structure that elevates as a single unit upon levator contraction. The preseptal skin, in contrast, is nonadherent and thus relatively mobile. Levator contraction thus results in invagination of the unified pretarsal unit beneath the mobile preseptal skin, creating a pretarsal fold. This description of the lid fold mechanism is consistent with the fact that in eyelids lacking a well-defined fold, the pretarsal skin is redundant because of an absence of attachments to pretarsal muscle and tarsal plate. Surgical procedures for creation of a superior palpebral furrow achieve this goal in spite of the fact that they were conceived based on the previously described anatomic oversimplification. Creation of an adhesion between the pretarsal dermis and levator aponeurosis or tarsus1 effectively produces an adhesion at the point of fixation, thus creating the boardlike unit that invaginates beneath preseptal skin on levator contraction. A more stable adhesion can be formed by undermining pretarsal skin 1 to 2 mm inferiorly prior to fixation, a maneuver that I accomplish by excision of a strip of pretarsal orbicularis oculi muscle. Figure 2-4 Anatomy of the Asian (“single eyelid”) upper eyelid. The anatomy of the periorbital fat compartment differs in the Asian upper lid as compared with the Caucasian lid (Figs. 2-3, 2-4). In both, the periorbital fat compartment is enclosed by the orbital septum, but in the Asian lid, because of the lack of preseptal adhesions, the periorbital fat compartment descends inferiorly, coursing a variable distance anterior to the tarsal plate. The more inferior location of periorbital fat and the increased amount of subcutaneous and suborbicularis fat are responsible for the characteristic puffiness of the “single” eyelid. In conjunction with redundant pretarsal skin, this fat abundance imparts an impression of diminished width of the palpebral fissure and occasionally produces a suggestion of ptosis (pseudoptosis orientalis). This wedge of fat descending anterior to the tarsal plate must be removed surgically to achieve fixation as it serves as a barrier between pretarsal skin and the lid opening mechanism. A third difference between the Asian and Caucasian upper eyelid is the epicanthal fold, a structure that is present in ~90% of East Asians. There is substantial variation in the size and configuration of the epicanthus, and if large, this weblike structure blunts the medial canthus, obscures the lacrimal caruncle, and is associated with diminished length of the palpebral fissure as well as diminished intercanthal distance that produces an aesthetically undesirable widening of the nose. Surgical modification of the epicanthus is often a goal of Asian blepharoplasty even in cases in which westernization is not desired; some patients request this procedure to improve nasal aesthetics. The desires of patients requesting double-eyelid surgery vary tremendously. Many patients request only creation or enhancement of a superior palpebral fold, wishing to retain other characteristics of the Asian lid, whereas others prefer more extensive transformation; the amount of skin and fat removed during surgery varies accordingly. In this regard, the ability to translate individual patient desires into an operation that reliably sculptures the upper eyelid to each patient’s general specifications is a major asset for the aesthetic surgeon. Preoperatively, patients are counseled that three basic decisions are necessary prior to surgery: As a starting point, eyelid size is arbitrarily characterized as small, medium, or large and eyelid shape as round or oval. Perhaps the best method of communication regarding eyelid size and shape involves examination of pre- and postoperative photographs that illustrate the basic sizes and shapes of eyelids (Figs. 2-5 to 2-10). Another method of demonstrating eyelid size and shape is manipulation of the eyelid skin with a bent paper clip (or an instrument especially designed for this purpose available from Asian surgical supply companies) while the patient is looking into a mirror. Some patients bring photographs of magazine models to their consultations. Although it must be stressed that the surgeon cannot construct an eyelid to the patient’s exact specifications, examination of these images in conjunction with actual pre- and postoperative photographs often facilitates determination of the general size and shape of eyelid that the patient desires. Figure 2-5 (A,B) Surgical creation of a small, round double eyelid with an inside fold. The incision was placed 6 mm above the ciliary margin, and 3 mm of skin was excised. Figure 2-6 (A,B) Surgical creation of a small, oval double eyelid with an inside fold. The incision was placed 7 mm above the ciliary margin, and 3 mm of skin was excised. Note the rudimentary left double eyelid characterized by a shallow palpebral fold and pretarsal skin laxity with inferiorly oriented eyelashes. It would be unwise to operate only on the right eye in an attempt to match the left eyelid because a surgically created fold will not assume the characteristics of the rudimentary natural fold. Figure 2-7 (A,B) Surgical creation of a medium, round double eyelid with an outside fold. The incision was placed 8 mm above the ciliary margin, and 50% of the maximum amount of skin that could be removed (as determined by forceps pinching) was actually removed. Note the rudimentary double eyelids for which the patient requested surgical enhancement. Figure 2-8 (A,B) Surgical creation of a medium, oval double eyelid with an inside fold. The incision was placed 8 mm above the ciliary margin, and 50% of the maximum amount of skin that could be removed (as determined by forceps pinching) was actually removed. In discussing modification of the epicanthal region, pre- and postoperative photographs are exceedingly helpful in demonstrating the difference between the so-called inside and outside fold (Fig. 2-11) and enables a meaningful discussion of possible surgical variations. Figure 2-9 (A,B) Surgical creation of a large, round double eyelid with an outside fold. The incision was placed 9 mm above the ciliary margin, and the maximum amount of skin that could be removed as determined by pinching the skin with forceps, less 3 mm, was actually removed. Figure 2-10 (A,B) Surgical creation of a large, oval double eyelid with an outside fold. The incision was placed 10 mm above the ciliary margin, and the maximum amount of skin that could be removed as determined by pinching the skin with forceps, less 3 mm, was actually removed.
Asian Blepharoplasty
♦ Upper Blepharoplasty


Anatomic Considerations


Preoperative Considerations






Preoperative Planning
| See DVD Disk One, Marking the Eyelid: Design and Planning |  |
Because postoperative asymmetry is by far the most common reason for patient dissatisfaction, the key to success in Asian upper blepharoplasty is to perform each and every step (from preoperative marking to final suturing) with the express goal of achieving eyelid symmetry. Two variables controlled by the surgeon determine the level or height of the superior palpebral fold that is eyelid size (small, medium, or large), the first being the distance from the ciliary margin at which the inferior lid incision is made. This level ranges from 6 to 10 mm above the ciliary margin, depending on the eyelid size desired. The second variable that determines eyelid size is the amount of preseptal skin that hoods over the surgically created palpebral fold and pretarsal skin postoperatively. In other words, pretarsal show determines actual lid size; as the amount of overhanging skin increases, pretarsal show decreases (and the lid appears smaller), and vice versa. It should be obvious that the amount of preseptal skin available to hood over pretarsal skin is determined by the amount of skin that is excised above the surgically created palpebral fold, a factor that is determined by the level of the superior incision.

Figure 2-11 The left eye exhibits an outside fold (epicanthal effacement), and the right eye exhibits an inside fold (no epicanthal effacement).
Putting these two variables together allows creation of a formula or system, the utilization of which allows reliable construction of a small, medium, or large upper eyelid (Table 2-1).
The shape of the eyelid can be controlled by the configuration of the inferior incision. To create an eyelid with an oval shape, the incision is drawn so that it is at approximately the same height (distance from the ciliary margin) at the lateral limbus as at the lateral canthus. If a round eyelid shape is desired, the lateral aspect of the incision is drawn so that it is ~2 mm more inferior at the level of the lateral canthus than at the level of the lateral limbus. In either case, the incision is then extended laterally as far as necessary so that it will fall in a lateral periorbital line, just as in Caucasian blepharoplasty.
| Size | Distance from Ciliary Margin (inferior incision) | Amount of Skin Excision (superior incision) |
| Small | 6–7 mm | 3 mm |
| Medium | 8 mm | 50% of maximum amount* |
| Large | 9–10 mm | maximum amount −3 mm* |
The patient’s desires regarding management of the epicanthal region determine the configuration of the medial aspect of the incision. If an inside fold is requested, the incision is drawn lateral to the existing epicanthus (Fig. 2-12A). If an outside fold is desired, the incision terminates medial to the epicanthal web (Fig. 2-12B). Many patients request a “compromise” fold, in which the lateral aspect of the epicanthus is effaced while the origin is preserved. In such cases, the medial aspect of the incision is placed so that it terminates on or near the epicanthal origin (Figs. 2-12C, 2-13A,B).
Proper preoperative markings are critical for achieving surgical success. Prior to marking the inferior incision, it is extremely important to tense the lax pre-tarsal skin cephalically to the point of slight eyelash eversion. If this is not done, surgical fixation is likely to result in a palpebral furrow that is higher than planned or unattractive postoperative fullness of the pretarsal skin. A mark in the depression located just superior to the ciliary margin (placed at midpupillary level) assists in symmetrical marking of the inferior incision. The distance above the ciliary margin can be measured from this mark with a caliper or ruler.

Figure 2-12 (A) Incision used for creation of an inside fold. (B) Incision used for creation of an outside fold. (C) Incision used for creation of a fold terminating on the origin of a small epicanthus (compromise fold).

Figure 2-13 (A,B) Surgical creation of a medium, oval double eyelid with a compromise fold.
Before marking the superior incision, the maximal amount of skin that can be excised is determined by pinching the skin with forceps and asking the patient to open and close the eyes as done in standard Caucasian blepharoplasty. The actual amount of skin to be removed, however, is determined by reference to the formula (Table 2-1), and the superior incision is marked at this level. It is imperative to understand that, although the usual Asian eyelid exhibits considerable skin redundancy, and even in the teenage patient the maximum amount of skin that can be removed frequently exceeds 10 mm, a much more conservative skin excision (as indicated by the formula) is necessary in all patients except those who truly desire westernization. After determining its proper level, the superior incision is marked so that it parallels the inferior incision, tapering to join the inferior incision at its medial and lateral termini.
A third variable to be considered in preoperative planning is the amount of fat, primarily periorbital, that requires removal. Although of paramount importance in determining the depth of the palpebral sulcus, the extent of lipectomy has a definite influence on lid size. As progressively larger amounts of fat are resected, increasing concavity is created into which preseptal skin invaginates, making less of this skin available to hood over the palpebral fold, thus increasing the amount of pretarsal show that determines eyelid size. For this reason, unless westernization of the eyelid is planned, fat removal in Asian blepharoplasty is more conservative than in Caucasians.
Anesthesia
Surgery is performed under local anesthesia (1% lidocaine or 0.5% bupivacaine freshly mixed with epinephrine (1:50,000) administered following intravenous sedation. Because the patient is asked to open and close the eyes at frequent intervals during placement of fixation sutures to evaluate symmetry, general anesthesia is not recommended. For the same reason, the level of sedation during surgery should be light. Diazepam and midazolam are best avoided, as both agents may interfere with voluntary lid opening. Use of intravenous methohexital or propofol just prior to infiltration of local anesthetic yields excellent results, as the patient is hypnotic and amnestic during anesthetic injection and sufficient residual sedation persists during surgery.
Operative Procedure
| See DVD Disk One, Double-Eyelid Blepharoplasty: The Full-Incision Approach |  |
A step-by-step description of the operative procedure follows:

Figure 2-14 Skin is excised, exposing the orbicularis muscle.
- Skin and underlying subcutaneous tissues are excised as marked, exposing the orbicularis muscle (Fig. 2-14).
- A 3 to 5 mm strip of orbicularis is excised above the level of the tarsal plate, exposing the orbital septum (Fig. 2-15).
- The orbital septum is incised, affording access to periorbital fat (Fig. 2-15). In contrast to the thin, filmy septum that characterizes most Caucasian lids, in many Asian eyelids the orbital septum is relatively thick, having a glistening white appearance that can be confused with the levator aponeurosis. The inexperienced surgeon is even more likely to confuse the orbital septum with the levator aponeurosis in patients who exhibit substantial amounts of submuscular fat, creating the impression that this fat represents periorbital fat, and the glistening white layer posteriorly therefore must be the levator aponeurosis. The periorbital space should be entered as superiorly as possible to minimize the possibility of injuring the levator aponeurosis. The extent of lipectomy depends on the type of eyelid transformation planned. If a small double eyelid is the surgical goal, only sufficient fat to allow accurate identification of the tarsal plate/levator aponeurosis is removed. If a large westernized eyelid has been requested, removal of substantial amounts of fat in the central and lateral compartments is performed as in Caucasian blepharoplasty so that the levator expansion is completely cleared. Construction of a medium-sized lid dictates lipectomy between these extremes. In all cases, however (including westernization procedures), removal of fat in the medial compartment must be very conservative, as creation of a deep hollow in the medial aspect of the lid does not produce the aesthetically desirable effect that results from sculpturing this area in the Caucasian eyelid. Excessive fat removal medially also predisposes to hypertrophic scarring in this area, as more tension on the skin closure results. In contrast, care must be taken to ensure that the point of fixation (tarsus/levator aponeurosis) is adequately cleared in the lateral aspect of the eyelid, as this is the most common area for early failure of a fixation suture resulting in localized fold loss or inadequacy. Even if a small double fold is to be constructed, the surgeon must ensure that periorbital fat and orbital septum, which is more substantial laterally, is adequately removed in the lateral aspect of the eyelid.
- The wound has now been prepared for placement of fixation sutures, but prior to their placement, a 2 to 3 mm strip of pretarsal orbicularis is removed from beneath the skin at the level of the inferior skin incision (Fig. 2-16). This maneuver is performed for two reasons: (1) the pretarsal skin is effectively undermined 2 to 3 mm providing a wider base for the adhesion creating the palpebral fold, and (2) this undermining allows more effective tightening of pretarsal skin during fixation, reducing postoperative laxity.
- External fixation sutures of 5-0 nylon are then placed, sequentially incorporating the skin edge of the inferior incision, the levator aponeurosis/tarsus at the desired point of fixation, and the superior skin incision, each suture being tied externally (Fig. 2-17A). In determining the point of fixation, the pretarsal skin is stretched cephalically just to the point of beginning eyelash eversion; having a constant reproducible end point is important in achieving eyelid symmetry. Buried internal fixation sutures (Fig. 2-17B) of permanent or absorbable material incorporating only the inferior skin incision and levator/tarsus may be substituted for the “external” fixation sutures, but including the upper skin edge in the fixation process provides a major advantage as it enhances intraoperative determination of symmetry because the precise effect of hooding contributed by the preseptal skin is more easily assessed. Three fixation sutures are routinely used, being placed (1) laterally at a point approximately half the distance between the lateral canthus and lateral limbus, (2) centrally at the mid-pupillary level, and (3) medially at the level of the medial limbus (Fig. 2-18A,B). Assessment of symmetry is greatly enhanced if the sutures are placed sequentially in the right and left eyelids; that is, the lateral fixation suture is placed in the right upper lid, following which a matching lateral fixation suture is placed in the left lid. The patient is asked to open his or her eyes, and symmetry is assessed by inspection and direct measurement. If absolute symmetry is not present, one of the fixation sutures is removed and replaced, allowing symmetry to be achieved. In a similar fashion, the middle fixation suture is placed in the right and then the left eyelid, following which symmetry is again assessed. The medial fixation sutures are then placed sequentially, and the lids are examined for symmetry. In many cases, one or two additional medial fixation sutures are placed following undermining of the pretarsal skin in this area to modify the epicanthal fold. Such medial advancement of the epicanthal fold by undermining and fixation sutures satisfies the desire of most contemporary patients with respect to epicanthoplasty. On occasion, however, more advanced techniques of epicanthal effacement described in a later section are used.
- The entire incision is then approximated with a running suture of 6-0 nylon. Use of absorbable suture material for skin closure often results in prolonged erythema of the incision and thus is not recommended. Many surgeons advocate the use of a running subcuticular suture for upper lid closure, but placement of such a suture places the fixation sutures at risk both intraoperatively and at the time of removal.
- Following this, 0.2 cc of triamcinolone (10 mg per cc) is injected subcutaneously in the medial aspect of the wound. This area exhibits a biological predisposition for hypertrophic scar formation even in the absence of significant epicanthal modification, and prophylactic treatment with triamcinolone greatly reduces the incidence of induration and/or hypertrophic scarring in this region.

Figure 2-15 Following skin excision, a 3 to 5 mm strip of orbicularis is excised in the superior aspect of the wound, i.e., above the level of the tarsal plate, exposing the orbital septum. Incision of the orbital septum affords access to the periorbital fat and following lipectomy, the levator aponeurosis is identified. Care must be taken to avoid confusing the orbital septum with the levator aponeurosis.

Figure 2-16 Following lipectomy and prior to placement of fixation sutures, a 2 to 3 mm strip of pretarsal orbicularis is removed at the level of the superior tarsal margin.

Figure 2-17 (A) External fixation suture. (B) Internal fixation suture. External fixation sutures are preferred for reasons ascribed in the text.

Figure 2-18 (A) Three (lateral, middle, and medial) fixation sutures have been placed. (B) The double eyelid is noted on lid opening following fixation suture placement.
Special Considerations and Variations in Asian Upper Blepharoplasty
Preexisting Small Double Eyelid
A substantial number of Asian patients who request upper-lid blepharoplasty present with an existing double eyelid. Many of these individuals have small natural double lids, and others have undergone previous eyelid surgery but are unhappy with the size or shape of the surgically created lid. It is not uncommon for an Asian patient to exhibit a small unilateral double lid, having a typical single lid on the contralateral side. Surgeons should resist requests by such patients to perform surgery on the single eyelid only, as it is difficult to achieve symmetry in these cases unless bilateral surgery is performed (Fig. 2-19A,B).

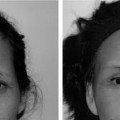
Figure 2-19 (A,B) Pre- and postoperative results in a patient with a preexisting unilateral double eyelid who underwent bilateral upper blepharoplasty rather than attempting unilateral surgery on the single eyelid only.
Regardless of the etiology of the problem, the goal of upper-lid blepharoplasty in this group is usually to enlarge the existing lid, deepen the sulcus, and/or change the shape of the lid from round to oval (or, rarely, from oval to round). Additional benefits of surgery include tightening of the preseptal skin and eversion of the eyelashes into a more aesthetically pleasing orientation. Upper blepharoplasty allows enhancement of lid aesthetics by enabling more effective use of cosmetics that provide transformation of the sad, tired appearance often imparted by small lids to a more “bright-eyed” look (Fig. 2-20A,B).
The surgical procedure in such patients is conducted according to the guidelines described above, the level of the inferior incision and extent of skin removal depending on the eyelid size and shape desired. Of utmost importance, however, is the observation that in most natural double eyelids, the pretarsal skin exhibits considerable laxity, and thus the inferior incision must be placed inferior to the existing fold (the actual location being determined by cephalic traction on the eyelid skin as previously described).

Figure 2-20 (A,B) Pre- and postoperative results in a patient with preexisting natural double eyelids who requested a larger upper eyelid with a more well-defined palpebral fold.
The Aging Asian Eyelid





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


