Stage I
Asymptomatic
Stage II
Claudicatio intermittens
Walking distance:
IIA
>200 m, with no disablement
IIB
< 200 m with disablement
Stage III
Resting pain
Stage IV
Peripheral necrosis/gangrene
35.3 Clinical Findings
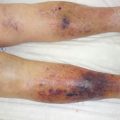
The typical localization for arterial leg ulcers is the lateral malleolar region for PAOD stage IIB (Fig. 35.1), whereas distal arterial necrosis (PAOD stage IV) is usually localized in the foot and toe region (Fig. 35.2). Arterial leg ulcers often have irregular edges and/or a “punched-out” appearance. The ulcer base is usually poorly developed with a grayish granulation tissue. Signs of chronic venous disease are missing except in mixed ulcers. Painful and necrotic areas are the typical appearance for all ischemic ulcers.


Fig. 35.1
Typical arterial leg ulcer on the lateral malleolar aspect of the lower leg (PAOD complicated stage IIB)
Fig. 35.2
Distal arterial necrosis due to PAOD stage IV
35.4 Diagnosis
The first test to rule out arterial insufficiency should be the palpation of the pedal pulses. It should be mentioned that the dorsalis pedis pulse is missing in about 10 % of individuals and the palpation of the posterior tibial pulse may be difficult due to swelling or the presence of ulceration caused by a concomitant chronic venous insufficiency. If a pulse is palpable, we can assume that the ankle pressure is >100 mmHg [13] and wound healing should be possible. If no pulses can be detected, noninvasive vascular testing should always be performed.
As a fast and simple test, the ankle-brachial index (ABI) can be measured very easily with a cheap and simple continuous wave (CW) Doppler probe (8–10 mMHz). The ABI is defined as the systolic ankle pressure divided by the systolic arm pressure and is considered an accurate and reliable marker of symptomatic and asymptomatic PAOD (Table 35.2). Significant arteriopathy is normally defined as an ABI <0.91 and an ABI <0.5 as severe arterial insufficiency [23]. The ABI measurement can therefore identify patients at risk of any systemic atherothrombotic events even in an asymptomatic stage. Identification of asymptomatic PAOD also leads to intensified targeted prophylactic anti-atherothrombotic treatment that can reduce morbidity and mortality as mentioned above [8].
0.91–1.4 | Normal, if under exercise no ABI loss |
0.5–0.85 | PAOD, claudication (mild to moderate disease); a wound can heal |
<0.5 | Severe PAOD, threat of tissue and limb loss |
>1.4 | May be due to diabetes, Mönckeberg disease, renal disease |
To recognize critical ischemia the measurement of ankle systolic pressure is the most accurate test. If the pressure is below the level of critical limb ischemia as defined with an ankle systolic pressure <50 mmHg [14], leg ulcers will only heal in 20 % of cases, and aggressive revascularization therapy should be performed [15]. In contrast, a systolic pressure over 70 mmHg can nearly exclude arterial insufficiency as a cause for the ulcers. If the arteries are not compressible, i.e., the ABI is higher than 1.4 or the difference of the measured pressure between ankle and arm exceeds 75 mmHg, calcification of the arteries should be considered. In these cases, a toe systolic pressure or a tcPO2 measurement should be performed. In cases of Mönckeberg mediocalcinosis, the pole test technique can also give further information concerning the critical ischemia of the lower limbs. A toe systolic pressure lower than 50 mmHg or a tcPO2 lower than 30 mmHg is diagnostic for critical ischemia (Table 35.3). If the tcPO2 is over 30 mmHG, a wound can heal. Ultrasonic duplex scanning or arteriography can localize the arterial lesion but cannot make any statement about the severity of the arterial disease. In contrast, it is a very good surveillance tool after an invasive intervention or as first-step screening in order to evaluate an invasive procedure. The gold standard to investigate PAOD is still angiography, especially when an intervention is planned. Recently, magnetic resonance angiography has emerged as a noninvasive imaging modality without the risks associated with conventional angiography (e.g., arterial puncture, plaque embolization, and contrast-induced nephropathy).
Table 35.3
Use of noninvasive vascular tests to predict the presence of underlying severe arteriopathy [22]
Noninvasive ascular testing | Findings | Severearteriopathy |
|---|---|---|
Pedal pulses | Present | Unlikely |
Absent | Possiblea | |
Ankle systolic pressure | >70 mmHg | Unlikely |
With ulcer | < 50–70 mmHg | Possiblea |
Without ulcer, withrest pain | <30–50 | Likely |
Toe systolic pressure | >50 mmHg
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|