(1)
Hôpital Universitaire de Strasbourg, Strasbourg, France
Abstract
All lesions described so far may also include an alteration of the surface of the skin and thus produce intricate lesions (e.g., a papule may become necrotic = necrotic papule). Some lesions known as “primary,” with an initially normal surface, will evolve towards an alteration of the skin surface. This observation explains the historical designation of “secondary lesions” for skin surface alterations. However, it is an inaccurate term since these lesions can be initially present in numerous conditions and are not necessarily an evolution of a “primary lesion.” For teaching purposes, these lesions have already been defined and briefly covered in Chap. 2. A more comprehensive description is presented here, although readers may also refer to the illustrations in Chap. 2.
All lesions described so far may also include an alteration of the surface of the skin and thus produce intricate lesions (e.g., a papule may become necrotic = necrotic papule). Some lesions known as “primary,” with an initially normal surface, will evolve towards an alteration of the skin surface. This observation explains the historical designation of “secondary lesions” for skin surface alterations. However, it is an inaccurate term since these lesions can be initially present in numerous conditions and are not necessarily an evolution of a “primary lesion.” For teaching purposes, these lesions have already been defined and briefly covered in Chap. 2. A more comprehensive description is presented here, although readers may also refer to the illustrations in Chap. 2.
Normal skin is smooth and dry (except for sweat), and the microrelief is apparent. Soft scratching using a Brocq’s curette (or otherwise rubbing with the finger or a black piece of cloth) does not cause scale removal.
The standard terminology for these alterations of the skin surface is as follows.
7.1 Skin Surface Is Too Thin
7.2 Skin Surface Is Thickened
The skin then becomes yellow, hard, and rough.
Keratosis is defined as a thickening of the stratum corneum, which is broader than thick (cf. Figs. 2.3 and 7.1). From a clinical point of view, it is characterized by circumscribed or diffuse lesions, very adherent and hard on palpation. The feeling on palpation is very peculiar because keratosis confers a rigid hard effect to the skin which turns out to be inflexible under finger pressure. A feeling of roughness can also be noted on rubbing. Skin exploration using the curette confirms this feeling of hardness; it is almost impossible to remove any scales.
A cutaneous horn is a thicker keratosis, which is more elevated than broad (Fig. 7.2).
A millimeter-wide, punctuate keratosis, covering and infiltrating the hair follicles, is called a horny plug (Fig. 7.3).
Finally, certain lesions known as porokeratoses are well demarcated and lined by a fine, keratotic collarette, which is very typical, elevated, and adherent (Fig. 7.4).

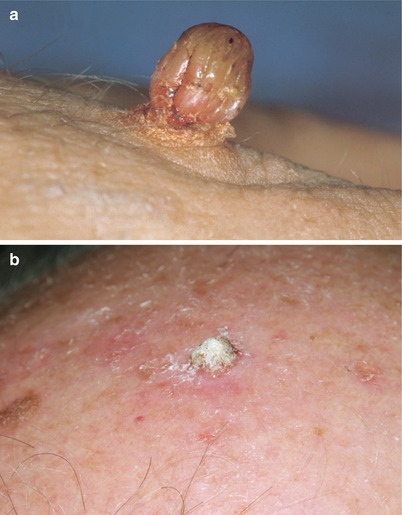


Fig. 7.1
Keratosis. Callosity. Keratosis corresponds to a thickening of the stratum corneum, which is more horizontally spread (superficially) than vertically raised (in height). In contrast, a cutaneous horn (cf. Fig. 7.2) is a keratosis that is more elevated than superficially spread. Keratosis and cutaneous horn are rough and adherent lesions, not easily dislodged and causing bleeding upon removal, as opposed to scales and crusts. In callosities, there is thickening of the stratum corneum producing a thickening, roughness, and yellow appearance of the skin. Note that the cutaneous microrelief including epidermal ridges (dermatoglyphs) is perfectly left intact, as opposed to other keratotic lesions such as plantar warts (cf. Fig. 12.55)
Fig. 7.2
Cutaneous horn. Warts. Actinic keratosis. (a) Exophytic lesion of the stratum corneum (pointing outwards) corresponding to a wart. (b) The horn is located on a red lesion, barely elevated and identified on its borders. The lesion is an actinic keratosis, which is a very superficial squamous cell carcinoma (cf. Chap. 13). Also note the skin of the scalp. It is red and brown and covered with numerous actinic keratoses, which illustrate the concept of field cancerization
Fig. 7.3
Follicular horny plugs. Chronic lupus erythematosus. Note the follicular distribution of keratotic papules on a leukodermic plaque with erythematous borders. These horny plugs are very adherent. They are typical of chronic lupus erythematosus but may be seen in other disorders such as seborrheic keratoses or superficial pemphigus
Fig. 7.4
Keratotic collarette (arrow). Porokeratosis. This lesion is lined with a very adherent and fine keratotic collarette, which can be felt on palpation
7.3 Skin Surface Is Absent
In this case, the skin becomes humid, oozing, serohemorrhagic, or fibrinous. These lesions are separated according to their depth. An erosion is a loss of the superficial part of the skin or epidermis, and it heals without leaving a scar (cf. Figs. 5.8 and 7.5). It is a humid and weeping lesion, secondarily covered by a crust and set on a bed of numerous red spots (0.1–0.2 mm) which correspond to the dermal papillae.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


