ANATOMY AND PHYSIOLOGY OF THE EYELIDS
John L. Wobig and Roger A. Dailey
STRUCTURAL PLANES OF THE EYELIDS
Although the anatomist may divide both upper and lower eyelids into eight layers, the surgeon, for more practical purposes, may divide them into five structural planes: (1) the skin and subcutaneous fascia, (2) the protractors of the eyelids, (3) the orbital septum, (4) the retractors of the eyelids, and (5) the tarsi and conjunctiva. The ocular retinaculum, although not a structural plane, is included because of its anatomical relationship to these structures medially and laterally.
The medial and lateral connections of the various planes of the eyelids deserve special note as well. The ocular retinacula are important structures for the surgeon to consider during revision or reconstruction of the eyelids.
SKIN AND SUBCUTANEOUS FASCIA
The skin of the upper and lower eyelids is, with few exceptions, the thinnest in the body. The eyelid skin is unique in that it does not have any underlying subcutaneous fat. It is subjected to the most movement— stretching and relaxing with each blink.
Both the upper and the lower eyelids have transverse palpebral folds or furrows (Fig. 2-1). The superior palpebral furrow effectively conceals, postoperatively, the surgical approach to the inner structures of the eyelid. It denotes the dividing point between the loosely adherent preseptal skin and the more adherent pretarsal skin, and roughly marks the upper margin of the tarsus. Inferior to it, the fibers of the levator aponeurosis first begin to pass into the overlying pretarsal muscle and skin. Superior to it, the lower margin of the orbital septum attaches to the aponeurosis.
The furrow in the lower eyelid roughly marks the lower margin of the lower tarsus. It slopes from ~ 2 mm below the eyelash line medially to ~ 5 mm laterally.
PROTRACTORS OF THE EYELIDS
The beginning of a structure or organ in the body is called an anlage, a source, or an origin. In myology, a muscle grows from its origin and attaches at its insertion. This is true of all the skeletal muscles. The dictionary further states that the less movable end of a muscle is its origin. This is true of almost all muscles of the body except some of the superficial muscles of the face.
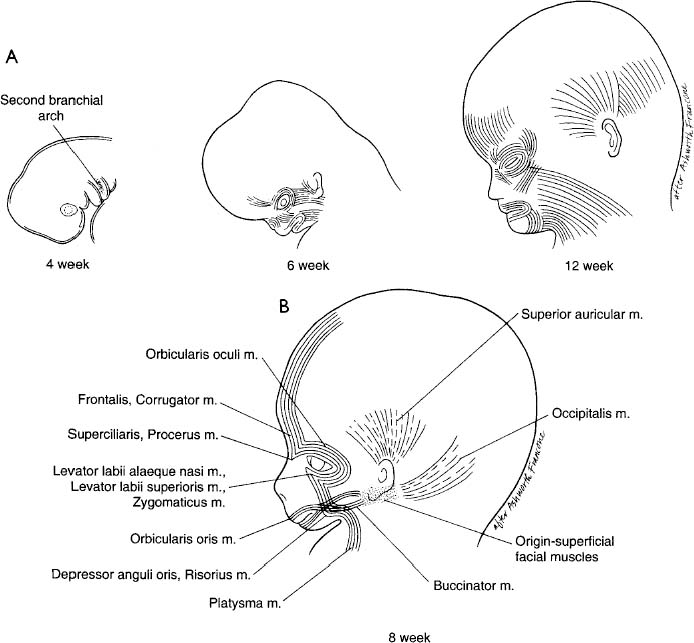
The anlage of all the superficial muscles of the ear, scalp, face, and neck is on the second branchial arch. The myoblasts of the occipital, external ear, and buccinator groups follow a normal pattern of growth. The muscles of the facial group, however, perhaps due to involutional changes in the second branchial arch, seem to be enabled to grow at each end, migrating down into the neck and upward to the scalp and forehead (Fig. 2-2A,B). As they mature, they reach their attachments on the bones of the head, the galea aponeurotica, the lacrimal diaphragm, and the subcutaneous fascia. It is our belief that the present use of the term origins of the facial muscles should be changed to insertions. Only then can the student decipher their embryology or understand their anomalies.
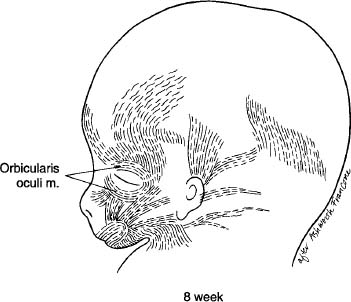
As the anterior part of the anlage migrates toward its insertions, the part that becomes the orbicularis oculi muscle bends around the orbit like a horse-shoe, inserting in the region above and below the medial canthus. Gasser stated that in the late myoblast stage (41 mm embryo), motor contraction begins (Fig. 2-3). The part that becomes the orbicularis oculi muscle is divided, somewhat arbitrarily, into orbital and palpebral parts, and the latter into preseptal and pretarsal parts (Fig. 2-4). These parts may act synergistically or independently; the orbital part being voluntary and the palpebral part being both voluntary and involuntary.
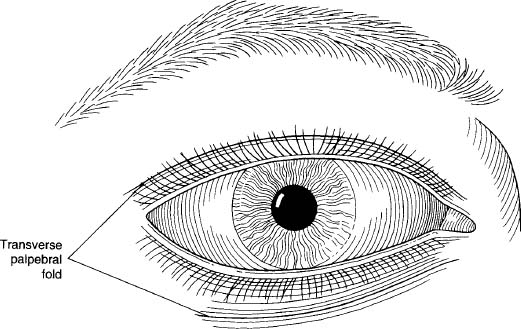
FIGURE 2-1 The skin of the upper and lower eyelids revealing the transverse palpebral folds.
The orbital part inserts below on the anterior aspect of the infraorbital bony margin, medial to the infraorbital foramen; above, it inserts on the anterior aspect of the supraorbital margin, medial to the supraorbital notch (Fig. 2-5).
The corrugator supercilii is actually a V-shaped muscle. In our anatomical dissections, we were able to trace a lateral bundle of muscle fibers of the frontalis from the highest point of its attachment to the galea-aponeurotica on down to the lower one-third of the body of the frontalis muscle. Here this bundle dips beneath the main muscle and continues obliquely to the medial end of the superciliary arch (Fig. 2-6). At this point it fuses with a downward curving bundle of muscle fibers from the orbital part of the orbicularis oculi muscle to make a common insertion there.
The procerus muscle and its lateral companion the superciliaris muscle are extensions of superficial frontalis muscle fibers and, from an embryonic point of view, “insert” on the nasal bone and frontal process (of the maxillary bone), respectively.
The preseptal parts of the orbicularis oculi muscle consist of the muscle bundles that make up the lateral palpebral raphe (Fig. 2-7). They extend medially above and below to the upper and lower medial canthal regions where they insert (Fig. 2-8). No true raphe exists laterally because the muscle bundles are not interrupted and do not inter digitate. The medial end of the lower preseptal muscle inserts mainly on the lacrimal diaphragm (Fig. 2-9). One muscle bundle often joins the medial canthal tendon posteriorly. A few muscle fibers (Merkel’s muscle) attach to the skin below the eyelid and insert with the lower preseptal muscle. The upper preseptal muscle inserts anteriorly to the upper margin of the medial canthal tendon, and posteriorly to the lacrimal diaphragm (Fig. 2-10). Its most posterior fibers may also insert on the posterior lacrimal crest.
The pretarsal muscles in both eyelids are firmly attached to the outer surface of the tarsi. The upper part of the upper pretarsal muscle is attached to the levator aponeurosis and, therefore, is separated to some extent from the upper part of the tarsus by the postaponeurotic space (Fig. 2-11). A common lateral canthal tendon (Fig. 2-12) attaches the pretarsal parts laterally to the lateral orbital tubercle. Except in primates, the muscle fibers themselves extend to the tubercle in all mammals.
Medially, the pretarsal parts divide into superficial and deep heads at the medial end of each tarsus (Fig. 2-13). The larger superficial heads include Riolan’s “pars ciliaris” of the pretarsal muscle (Fig. 2-14). The superficial heads unite to form the medial canthal tendon, which inserts on the medial orbital margin (only the nonprimate mammals have a true medial canthal ligament). The deep heads of the pretarsal muscle (Horner’s, Duverney’s tensor tarsi, pars lacrimalis) are formed by the fibers of the pretarsal muscles, which turn backward at the medial end of each tarsal plate, superior to the upper ampulla and inferior to the lower ampulla. They have a common interlacing insertion on the lacrimal bone behind the posterior lacrimal crest (see Fig. 2-13).
Both the superficial and the deep heads of the pretarsal muscles are firmly attached to the lateral part of each canaliculus. The upper superficial head attaches to the anterior side of the canaliculus, whereas the deep head attaches to the posterior side. In the lower eyelid, the superficial head attaches to the anterior side of the canaliculus, whereas the deep head attaches to the posterior-inferior side. The “submarginal muscle of Klodt” (pars subtarsalis) consists of fibers that probably arise from the ciliary part of the pretarsal muscle. The fibers lie posterior to the ducts of the tarsal glands (see Fig. 2-14). The submuscular fascia attached to the posterior surface of the orbicularis oculi muscle is fairly dense. It contains a network of the efferent branches of the facial nerve to the superficial facial muscle (Fig. 2-15). In it are small plexuses formed between it and the maxillary division of the fifth cranial nerve. It is thought that, when the facial nerve has been cut, as in bilateral blepharospasm or surgery on parotid tumors, these plexuses are involved in restoring the contractibility of the muscles.
Fibrous elements of fascia pass through the muscle bundles to the subcutaneous fascia, holding the skin firmly to the muscle in the pretarsal region and loosely in the preseptal region. In dermatochalasis of the upper eyelid, a mistaken belief is that a fold of skin can simply be picked up and cut off without cutting the underlying muscle. It is important to dissect the skin from the muscle. There is no fat between the septum and the submuscular fascia except that which is above in the region of the supraorbital margin. To separate the two layers from each other requires careful dissection.
ORBITAL SEPTUM
The orbital septum, together with the tarsus, represents the mesodermal layer of the embryonic eyelid fold. It is important as a surgical landmark and as the delineating structure between the orbit and the preseptal space. The two periosteal layers at the bony margin fuse and form a strong band, the arcus marginalis, of the septum. Fibers from the orbital fascia may also be found attached to the arcus. The septum forms an arch beneath the supraorbital notch and around the supratrochlear and infratrochlear nerves and vessels.
The septum fuses with the levator aponeurosis at varying levels, depending on the amount of fat in the preaponeurotic (postseptal) space. Most frequently, this occurs ~ 10 mm above the eyelid margin (Fig. 2-16). In the lower eyelid, the septum attaches to the lower margin of the tarsus and, except for a short distance from its attachment to the tarsus, is separated from the aponeurosis of the capsulopalpebral head by preaponeurotic fat.
Medially and below, the septum attaches to the spine (lacrimal tubercle) at the lower end of the anterior lacrimal crest. It then turns posteriorly behind the muscle attachments on the posterior lacrimal crest to become part of the upper orbital septum. Laterally, the septum dips posteriorly to the lateral canthal tendon where it loses its identity by fusion with the canthal tendon and the lateral horn of the levator aponeurosis.
RETRACTORS OF THE EYELIDS
The retractors of the eyelid serve to open the palpebral fissure to allow the eye to appreciate a wide visual field. Duke-Elder classified the orbital muscles as (a) extrinsic orbital muscle, (b) striated muscles of the eyelids, and (c) nonstriated orbital and periorbital muscles. A more practical description of these muscles of the eyelids would be to divide them into the upper and lower eyelid “retractors.”
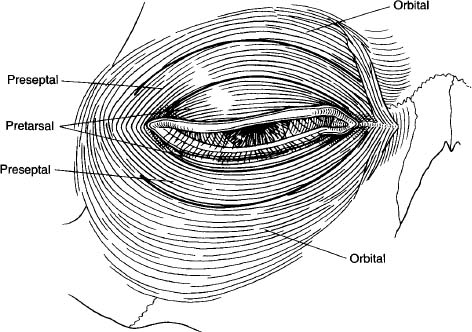
FIGURE 2-4 Orbicularis oculi muscle with its divisions into orbital, preseptal, and pretarsal parts.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


