Chapter 12 Alar Base Surgery
Online Contents
 Animations
AnimationsIn this Chapter Online at experconsult.com
Excision of Excess Nostril Sill Animation 12.1
Excision of Excess Nostril Sill and Alar Base Animation 12.2
Design of an Excision of Excess Lateral Alar Base Animation 12.3
Pearls
• Alar base incongruity can manifest as flaring of the nostrils with a wide alar base, alar base asymmetry, or an alar base that was improperly reduced causing an undesirable angulation and notching at the base of the ala.
• The alar base can also be malpositioned vertically, being either too cephalad or too caudal.
• The horizontal excess can be the result of a wide alar base, a thick alar base or a wide nostril sill, each of which will require a different type of surgical correction.
• A combination of horizontal and vertical excess or deficiency may coexist.
• When correcting the alar base excess related to the wide nostril sill, the incision is designed with almost parallel limbs at the nostril sill tapering laterally to the alar-facial crease.
• To eliminate the excess alar base width related to redundant nostril sill and wide alar base laterally, a combination of nostril sill and base excision is conducted using an elliptical incision.
• The lateral alar base excess is eliminated by designing an elliptical incision that is solely on the lateral portion of the alar base without extension to the nostril sill or the vestibular lining. The posterior limit of the incision will be placed in the alar-facial groove.
• The thick alar base is thinned and narrowed with an L-shape or crescent excision.
• An alar base can also be secondarily widened as a result of maxillary advancement or significant reduction of the tip projection which often requires a sill or combined excision.
• Moderate to severe cephalic malposition of the alar base is corrected by removal of an elliptical piece of skin from the upper lip, full mobilization of the ala, and caudal transposition of the alar base.
• If placement of an alar rim graft is intended, it should be inserted before alteration of the alar base since it can widen the nostril to some degree.
An imbalanced alar base is a common feature of an ‘operated nose’.1–3 This incongruity may manifest as flaring nostrils with a wide alar base that was not corrected during the primary rhinoplasty, alar base asymmetry, or, even worse, an alar base that was improperly reduced, thus eliminating the graceful transition from ala to nostril sill and causing a displeasing angulation at the junction of the alar base with the upper lip. This deformity can be difficult to correct. It is therefore essential to evaluate prudently the alar base abnormalities and plan the surgical correction with the utmost precision in order to avoid these undesirable outcomes. Additionally, understanding the dynamic interplays germane to the alar base surgery is absolutely crucial. This portion of the rhinoplasty should not be considered trivial and the role that the alar base surgery plays in the success of rhinoplasty is greater than is usually realized.
Anatomy and Pathology
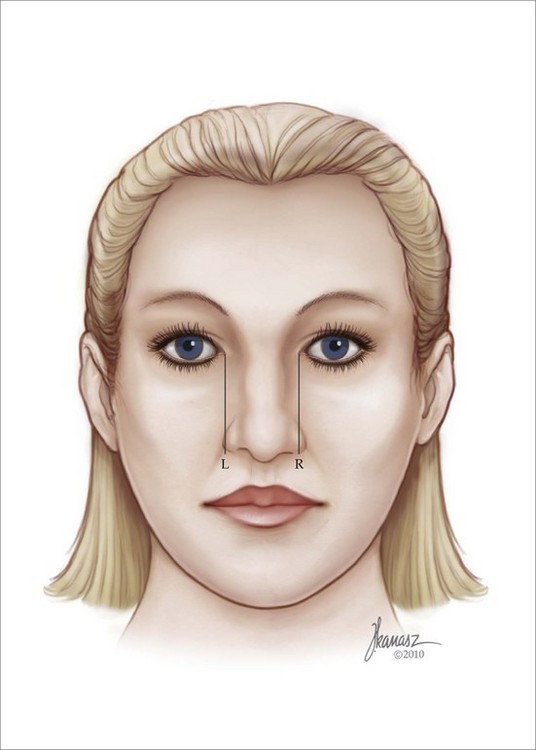
Recognition of alar base disharmony is the most important step in establishing a pleasing relationship between the base, the rest of the nose, and the face. The distance from the lateral limits of one alar base to the opposite side is approximately 2 mm wider than the intercanthal distance in a harmonious face. This is true as long as the intercanthal distance is optimal (normally 31–33 mm; Figure 12.1). Should the intercanthal distance be judged to be abnormal, the orbital fissure (the distance from the medial to lateral canthus) can be used as a guide to decide the width of the alar base. For analysis of this zone, as was discussed in Chapter 3, a vertical line dropped from the medial canthus in a nose with an optimal alar base should pass 1 mm medial to the outer boundary on each side of the alar base, as long as the intercanthal distance is normal.
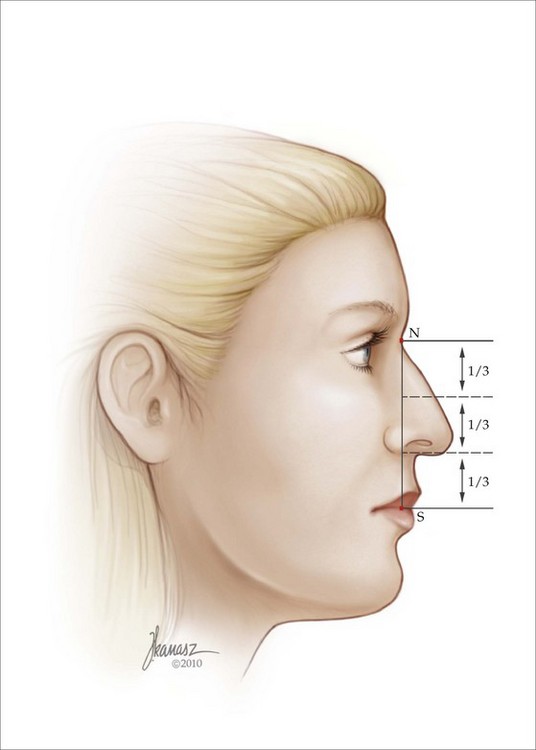
The vertical alar base position is readily determined on the profile view (Figure 12.2). Point N (nasion) is connected to point S (stomion) and the distance is divided equally into three. The caudal border of the alar base is located 2 mm caudal to the junction of the middle and lower thirds.
Alar base deformities can include horizontal excess (Figure 12.3), horizontal deficiency (Figure 12.4), or vertical malposition, which is either caudal (Figure 12.5) or cephalad (Figure 12.6




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


