11 Aesthetic Concerns in Transgender Patients
Summary
Keywords: transgender nonbinary gender affirmation nonsurgical cosmetic procedures minimally invasive cosmetic procedures noninvasive cosmetic procedures masculinization feminization
11.1 Background
11.1.1 Epidemiology of the Transgender Population
The prevalence of the transgender population has shown an upward trend, with study estimates reporting double the prevalence rates compared to a decade ago.1,2 One recent study reported about 0.6% of adults, approximately 1.4 million, and 0.7% of youth aged 13 to 17 years, or approximately 150,000 youth, identify as transgender in the United States.1 With the growth in the transgender population, medical providers including dermatologists must strive to improve their overall understanding, awareness, and knowledge in the medical care for this population.
11.2 Gender Transitioning
11.2.1 Overview: Medications and Surgical Procedures for Gender Transition
Gender transitioning refers to a process of aligning one’s gender presentation with one’s internal gender identity. Gender transitioning can occur on multiple levels, including social transitions, medical treatments, and/or surgical transformations.3 Social transitions involve using a preferred name and pronouns, and some may legally change their name.
The use of cross-sex hormone therapy for medical reassignment has become more commonplace in the transgender population.4 Transgender males (biologically female transitioning to male) may choose to undergo hormonal therapy with exogenous testosterone,4 which suppresses female secondary sex characteristics and masculinizes transgender men. The physical changes can begin within 3 months of initiating therapy, including medically induced menopause, changes in the distribution of fat on the face and body, enhanced muscle mass, and increased libido. Later changes include increased clitoral size, vaginal skin atrophy, and a deepened voice.4 Skin changes that occur with testosterone therapy include increased facial and body hair, increased oil production and acne, and male pattern hair loss.4 Nonbinary individuals may also choose to undergo medical therapy, by balancing hormones based on their personal goals.
For transgender females (biologically male transitioning to female), hormonal therapy includes hormonal supplementation with estrogen, with or without anti-androgen therapies like spironolactone or cyproterone acetate.4 The goal of therapy is to induce female secondary sex characteristics, including breast formation, fat redistribution, muscle mass reduction, testicular size decrease, and female patterned hair growth.4,5 The skin can become drier and thinner, with less oil production and smaller pore size. The rate at which these desired physical changes occur after hormonal therapy initiation varies, ranging from within a few months to 2 to 3 years.5 This rate will also depend on other factors, like genetics and age at which you start therapy. Although medical therapy alone may lead to significant visible changes (Fig. 11.1), some patients desire faster, more immediate, and more striking physical changes. Minimally invasive aesthetic treatments, which will be discussed in detail later, can be used to further enhance the desired feminine appearance by softening and balancing features, contouring the face and body, and providing more immediate results (Fig. 11.2, Fig. 11.3, Fig. 11.4, Fig. 11.5, Fig. 11.6, Fig. 11.7).

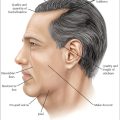
Fig. 11.1 (a) Before and (b) after hormonal therapy. Aesthetic changes include wider and more rounded convexities at temple and cheek. Also note the midface appears fuller with a softer and less angular contour through the mandible and chin.

Fig. 11.2 (a) Before and (b) after facial fillers in the same patient resulted in additional widening at the temple, cheek, and tear trough with a softer and more rounded contour to the mandible and chin. The lips are subtly enhanced to reveal a more natural, feminine lip projection with elevated mouth corners.

Fig. 11.3 (a) Before and (b) after laser hair removal to the lower face and neck, showing reduction in shadowing and softening of skin texture. This patient also received injectables to the upper face with botulinum toxin to smooth and gently arch the brow and facial fillers to the mid and lower face to enhance convexity of cheek, lips, and smooth contour of the mandible and chin. (c) After botulinum toxin injection to the masseter muscle, the face appears more heart shaped.

Fig. 11.4 (a) Before and (b) after injectable fillers to soften the temples, lift and smooth the depressed nasal root and reduce the prominent supraorbital brow ridges (with makeup removed). Additional lift to the brow was achieved after polydioxanone thread lifting, two treatments of microfocused ultrasound as well as botulinum toxin injection. (c) Before and (d) after with makeup showing the overall impact of upper face treatment as well as lower face. The lower face was treated with botulinum toxin injection to masseters to produce a more heart-shaped tapered jawline and fillers were used to enhance lip volume as well as lift the mouth corners and soften the chin/prejowl sulcus. Note that her lips will be treated in several sessions over time to gradually build volume while preserving a natural shape. (e) Before and (f) after oblique side angle showing the effect of lower face smoothing achieved with injectable facial filler, botulinum toxin, polydioxanone thread lifting, and laser hair removal.

Fig. 11.5 (a,b) The patient’s own “selfie” photos showing the before and after change achieved though minimally invasive aesthetic procedures including injectable fillers, botulinum toxin, microfocused ultrasound skin tightening, polydioxanone thread lifting, and laser hair removal.

Fig. 11.6 (a) Before and (b) after single-session treatment with little to no downtime. This patient received botulinum toxin to the glabella and injectable filler to lift the tear trough and enhance convexities of the cheek and temple.

Fig. 11.7 (a) Before and (b) after injectable botulinum toxin to the upper face and masseters to create a brow lift and more heart-shaped face with tapering at the jawline. Injectable fillers were placed to widen the temples and cheeks as well as lift the mouth corners and plump body of the lip. Laser hair removal was also started for the upper lip and chin.
Surgical gender reassignment procedures are also available for transgender patients in addition to medical therapy.5 Based on guidelines set by the World Professional Association for Transgender Health (WPATH) and the Endocrine Society, transgender patients should have undergone 1 year of hormonal therapy and living as the desired gender prior to gender reassignment surgeries.4 For transgender males, surgical options include oophorectomy, hysterectomy, scrotoplasty, phalloplasty, metoidioplasty, and chest masculinization surgery.6 Procedures available for transgender females include removal of the testes (orchiectomy), creating a neovagina (vaginoplasty), breast augmentation surgery, tracheal shave to soften the “Adam’s apple” (chondrolaryngoplasty), and voice feminization surgery. Facial plastic surgery is commonly pursued to soften facial contours, including rhinoplasty, fat transfer, forehead and chin implants, brow lift and forehead lift surgery, and orthognathic surgery.5 A population study published by Boston Medical Center between 2004 and 2015 reported 35% subjects had undergone at least one gender-affirming surgery, suggesting that the majority of transgender patients do not undergo any type of gender-affirmation surgery.7 This low rate may be due to multiple reasons, including paucity of providers, high financial cost, lack of interest, or aversion to invasive procedures.
11.2.2 Quality of Life Relating to Gender Identity and Aesthetic Procedures
Research has shown that transgender individuals report a low quality of life (QOL) and high incidence of mental health issues. In effect, medical and surgical gender-affirming surgeries are associated with higher QOL and high patient satisfaction.8,9 Despite this, even after transitioning, the transgender population continues to be at risk of lower QOL and mental health issues than the general population.10 Cosmetic concerns are especially tied to the emotional well-being of transgender patients because, by definition, their perceived gender identity and desired aesthetic presentation to the world differ from their biological sex. Improving the cosmetic appearance of transgender individuals based on their individual aesthetics may, in turn, further improve their QOL.
11.2.3 Barriers to Care
In order to improve access to medical care, providers must consider the many barriers transgender individuals face as they navigate the transition process. Barriers to good medical care include patients’ unfamiliarity with available procedures, paucity of trained providers in transgender health, delays while undergoing psychological evaluations, and high costs associated with required medications and surgical procedures. Additionally, distant location from metropolitan areas or large medical centers and lack of family or social support make access difficult for many patients. Medical providers may also become a barrier to good care. Physicians have the power to make themselves available or unavailable to transgender patients, provide transgender-friendly or transgender-unfriendly office environment, and to provide or delay prescriptions and cosmetic treatments at a pace that may not fit with the patient’s desired timeline. Board-certified providers may charge more money for procedures, and lack of insurance coverage for cosmetic procedures may be cost prohibitive for those patients without available resources. Confronted with societal pressures to conform to a binary gender system and ideals of beauty while faced with these barriers to receiving treatment, transgender patients may experience worsening anxiety, depression, and despair. Given these barriers, some patients pursue medical and aesthetic care beyond traditional medical providers,11 and may turn to illegal products, international internet prescriptions, or unlicensed or untrained providers. Unfortunately, cases of transgender patients resorting to “pumping,” or using liquid silicone, or receiving care from secondary providers have been reported,12,13 with associated complications. In contrast, it is optimal to receive aesthetic care from board-certified, trained medical physicians with experience in these procedures and dealing with the possible complications.
11.3 Improving Aesthetic Care through Minimally Invasive Aesthetic Procedures
11.3.1 Minimally Invasive Aesthetic Procedures
Clinical Pearl: Never assume you know what your patient sees in the mirror or what procedure they might be seeking. Dermatologists should ask their transgender patients vague questions to assess their unique concerns. Consider asking “tell me what concerns you have” or simply looking in the mirror and saying “tell me what you see.” Be sure to ask about what other treatments or procedures they are considering or have already planned so that you work within the framework of their overall transition with other physicians they might be working with (surgeons, psychiatrists, and endocrinologists).
Dermatologists can address specific cosmetic concerns including gender-affirming facial and body-contouring, hormone-related skin changes, and surgery-related scarring.14,15 Injectables, like botulinum toxin injections and filler treatments, are performed in an outpatient medical setting with minimal risk and little downtime compared to surgical interventions. Facial injectables can be started immediately to enhance or diminish certain features and to masculinize or feminize features according to patients’ aesthetic goals. Laser treatments and body-contouring devices are also available immediately and have high safety standards when performed by trained providers. With these noninvasive procedures, there is minimal need for psychologic vetting, medical pretreatment, or other delays that are routinely required prior to hormonal therapy and invasive surgery. They may also be more cost-effective for patients with more limited resources. In cisgender patients, minimally invasive aesthetic procedures have been shown to improve body image and QOL.16
Despite the growing medical literature regarding hormonal therapy and surgical procedures for gender transitioning, educational resources and published data regarding minimally invasive aesthetic procedures for transgender patients are sparse. Recently published reviews outline current dermatologic literature to instigate thought around this topic, but more detailed procedural outlines, case series, and larger studies on how dermatologists can contribute to the cosmetic transformation of the transgender patient would be helpful for the dermatologic community.14,15,17,18,19 Studies are currently underway to assess QOL data in transgender individuals who have received minimally invasive aesthetic services. Growing literature may cultivate an increased number of providers qualified and comfortable in performing aesthetic treatments in this population, thereby increasing access and QOL, as well as aid in future counseling efforts. The remainder of this chapter will review the role of medical providers, detail available minimally invasive cosmetic procedures relating specifically to the transgender population, and exhibit with our case examples.
11.3.2 Role of Dermatologists and Other Medical Providers
Dermatologists and other medical care providers should keep an open mind when assessing transgender patients for aesthetic procedures, as goals may be to feminize, masculinize, both, or neither. Transgender individuals’ aesthetic goals may diverge from the traditional gender paradigm of “masculine” or “feminine” ideals of beauty (Table 11.1).19,20,21 Accordingly, we advocate for a more flexible assessment of transgender patients. Practitioners should inquire about a patient’s individual goals during the initial consultation and throughout follow-up visits, listen to all patients, and discuss openly about their preferences, prior to proceeding with recommendations and treatments. As mentioned earlier, mental health issues remain a big issue in the transgender population. If any symptoms of mood changes or depression are detected, dermatologists should ensure that patients have a working relationship with a psychiatrist as well as strong social support.
Table 11.1 Traditionally “masculine” versus “feminine” facial features
Traditionally “masculine” features |
•Higher, possibly receding hairline •Wider more angular forehead •Flat horizontal brow •More prominent supraorbital brow ridges •Wider mouth with thinner lips •Longer, more square chin •Wider more square lower face •Beard hair or more coarse lower face skin texture •Acute nasolabial angle |
Traditionally “feminine” features |
•Lower hairline •Smooth, convex forehead •Brows arch above softer orbital rim •Eyes appear more open and/or wider set •Convex, prominent cheek contour •Heart-shaped, more tapered lower face •Smaller lower face to upper face proportion •Fuller vermillion contour and fuller lip body •More obtuse nasolabial angle |
As with all patients, the patient–physician relationship is important when dealing with transgender patients. Medical providers should avoid patronizing language regarding the patient’s decisions, listen deliberately, and develop an individualized plan to help moving forward with the transition process. The office medical forms should be comprehensive of all gender orientations, and clinical staff should also be trained to inquire and address patients with their preferred pronouns and names. With supportive care and better outreach, dermatologists can bring more transgender patients into the care of board-certified and trained physicians.
11.3.3 Patient Preferences
A recent cross-sectional survey study of 327 people showed that a majority of transgender men reported prioritizing their face as the most essential body part to have changed, over the face or genitals.14 These patients stated that they were mostly concerned about cosmetic procedures “looking good,” more so than the risk of scars, complications, or other risks. In contrast, transgender women reported their face as the most essential body part to have changed. Of facial procedures, transgender women stated hair removal was the most preferred cosmetic treatment, followed by surgery and then injectables.14 Transgender women reported seeking procedures mostly from plastic surgeons,14 which may be due to patient preference, prior physician relationship, better outreach, or ease of access.
It would be helpful to have before and after treatment photos of transgender patients who have undergone available dermatologic procedures available to help with outreach and to allow for transgender patients to relate to the subjects, rather than relying on results from cisgender patient images. We postulate that minimally invasive aesthetic procedures performed by dermatologists may become more common and sought after in both transgender men and transgender women with better outreach as well as additional literature on the available procedures, patient preferences, and typical outcomes.
11.4 Available Procedures and Illustrative Examples
11.4.1 Transgender men (female to male transition)
Transgender men benefit from dermatologic care and minimally invasive aesthetic treatments, and more awareness on available procedures is needed in the general public. As stated previously, transgender men report that their primary aesthetic concern is their chest, rather than their face or genitals. In our experience, pseudogynecomastia (residual breast tissue) posthormonal therapy with exogenous testosterone does not respond well to minimally invasive treatments like cryolipolysis (Fig. 11.8), and we routinely refer these patients for surgical correction. Noninvasive body contouring, like cryolipolysis and pulsed focused ultrasound, of other body areas, particularly in the abdomen, flanks, and submental regions, may be sought after and remains a good treatment option in transgender men.
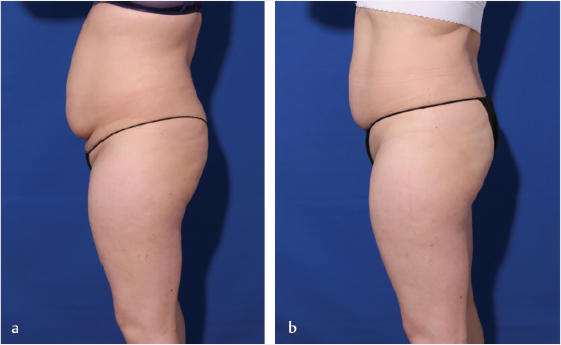
Fig. 11.8 (a) Before and (b) 2 months after abdominal cryolipolysis combined with three twice-monthly sessions of pulsed focused ultrasound in a transgender woman.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


