, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
27.1 Nevus Lipomatosus Superficialis
27.1.1 Clinical Features
Nevus lipomatosus superficialis is a rare benign cutaneous hamartoma. Two variants have been described. The classical form is present at birth or in the first 2 years of life. It presents as multiple soft, skin-colored to yellow papules and nodules that sometimes coalesce into plaques. Nevus lipomatosus superficialis is most common on the buttocks, lower back, and upper thighs [1]. A solitary type may appear in adulthood and is more likely to affect other areas of the body. These lesions are benign, and treatment is generally not necessary [2].
27.1.2 Histology
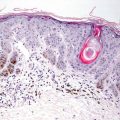
Nevus lipomatosus superficialis is characterized by a polypoid growth covered by normal-appearing epidermis. The dermis is remarkable for mature adipocytes extending high up into the dermis, admixed with normal-appearing collagen and cutaneous appendages [1]. There is often a mild perivascular inflammatory infiltrate consisting of lymphocytes and mast cells [3]. There are multiple reports of nevus lipomatosus superficialis occurring in association with other pilosebaceous hamartomatous proliferations [2, 4–6], vascular proliferations [7], and vascular anomalies [8].
The differential diagnosis of nevus lipomatosus superficialis includes acrochordon (skin tag). The presence of dermal-based fat is used as a distinguishing histologic feature in separating the two entities.
27.1.3 Pathogenesis
Some proposed mechanisms of the pathogenesis of nevus lipomatosus superficialis include metaplasia of adipocytes secondary to degenerative changes in the skin connective tissue, developmental displacement of adipose tissue in the dermis, and differentiation of lipoblasts around the blood vessels into adipocytes [9, 10]. It has been suggested that mutations in the PORCN (porcupine homolog) gene, which is involved in the processing of Wnt proteins, may have a role in the etiology of these lesions [11, 12].
27.2 Hibernoma
27.2.1 Clinical Features
Hibernoma is a rare tumor of brown fat, most commonly occurring in young adults [13]. Studies to determine sex predilection have been contradictory [13]. Hibernomas present as slowly expanding soft subcutaneous masses at the thigh or areas with higher density of brown fat deposition, such as the neck, axilla, back, and mediastinum. Lesions are benign and amenable to surgical excision with low rates of recurrence.
27.2.2 Histology
These tumors are usually located in the subcutis, but can appear within the reticular dermis [14]. They are comprised of multivacuolated fat cells with centrally placed scalloped nuclei [15] (Figs. 27.1 and 27.2). Several tumor variants including typical, myxoid, spindle cell, and lipoma-like have been described [13]. The typical type contains eosinophilic and pale cells . The myxoid variant has a loose, slightly basophilic stroma. The spindle cell type shares some histologic features with a spindle cell lipoma, and the lipoma-like variant is composed of primarily mature adipocytes with only scattered hibernoma-like cells. Mitoses are not common, and there is minimal cytologic atypia [16].
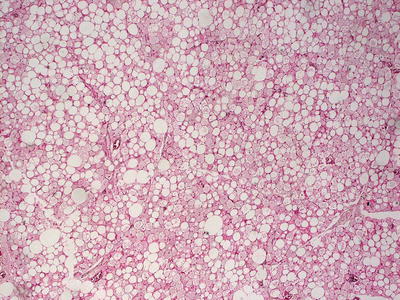
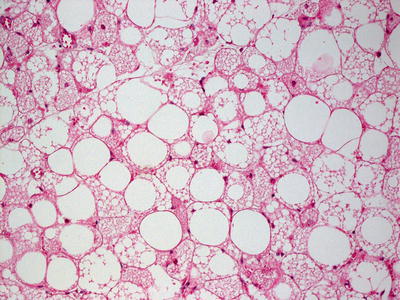
Fig. 27.1
Sheets of adipocytes with microvesiculation in the cytoplasm are seen in hibernoma
Fig. 27.2
Adipocytes demonstrate cytoplasmic microvesicles in hibernoma. No cytologic atypia is present
The histologic differential diagnosis is dependent upon the histologic subtype, and consists of spindle cell lipoma and typical lipoma. A sebaceous gland neoplasm is another differential consideration and it has a palisade of basaloid cells around tumor lobules that is not seen in hibernoma.
27.2.3 Pathogenesis
Hibernoma is a tumor of brown adipose tissue, which is rich in mitochondria and generates heat in response to cold exposure and food intake [13, 17]. In white fat, fatty acids are metabolized to produce energy in the form of adenosine triphosphate (ATP). In contrast, brown fat, owing to abundant mitochondria and thermogenin, metabolizes fatty acids into heat [18]. Brown fat is present in high abundance in neonates, and in decreased amounts in adults. Hibernoma often has chromosomal translocations involving chromosome band 11q13 [19, 20]. These aberrations have been shown to be associated with concomitant deletions of AIP and MEN1, which are two tumor suppressor genes that underlie the hereditary syndromes pituitary adenoma predisposition and multiple endocrine neoplasia type 1 (MEN1) [21]. Hibernoma has low expression levels of AIP and MEN1, and high expression levels of genes that are upregulated in brown fat (such as PPAR-α, PPAR-γ, PPARGC1A, and UCP1). It has been proposed that loss of MEN1 and AIP may be important for hibernoma development [21]. AIP functions as a repressor of peroxisome proliferator-activated receptor (PPAR)-α, and MEN1 regulates adipocyte differentiation through PPAR-γ [22, 23].
27.3 Lipoblastoma
27.3.1 Clinical Features
Lipoblastomas are uncommon soft tissue tumors, accounting for 1.6–3.1 % of soft tissue tumors in children less than 1 year old [24]. Over 80 % of cases occur before 3 years of age with 50 % diagnosed by one year of age, and include reports of congenital lesions [24]. Males are three times more likely to be affected than females, and most cases are reported in whites. Lipoblastomas are described as rapidly growing soft, nontender subcutaneous masses on the extremities [24]. Lesions are benign but clinically may mimic liposarcoma or other malignant soft tissue tumors. Therefore, tissue biopsy is prudent to confirm diagnosis. Definitive treatment is complete surgical excision as recurrence is frequently reported following incomplete excision.
27.3.2 Histology
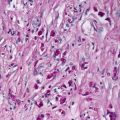
Lipoblastoma is a neoplasm that occurs in the dermis or subcutis. The tumor is composed of lobules of cells that show varying degrees of adipocyte maturation, and it is characterized by lipoblasts [25, 26] (Figs. 27.3, 27.4 and 27.5). Primitive stem cells are also present within the tumor cell population [25]. The lobules are irregularly sized and shaped, and can be well circumscribed or show an infiltrative growth pattern within the dermis and subcutis [26]. Well-defined septa separate the lobules of adipocytes [27]. There is an increase in vascularity, and a plexiform growth pattern has been described within the vascular proliferation [25]. A myxoid stroma is present [28]. Mitoses are rare or nonexistent [25, 26]. Diagnosis can be made on fine-needle aspiration cytology based upon the presence of lipoblasts and a myxoid matrix [29]. The absence of necrosis or mitotic activity in cytologic specimens is helpful in making this diagnosis.
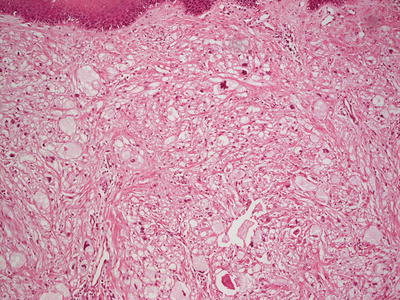
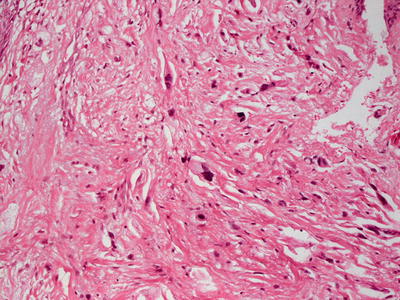
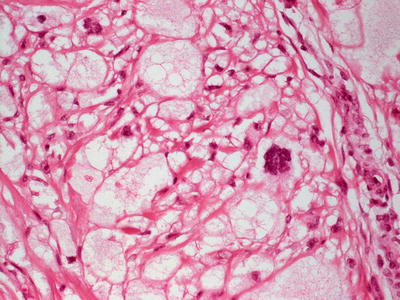
Fig. 27.3
Sheets of adipocytes are present throughout the dermis in lipoblastoma . They often appear to be diffuse and not well circumscribed
Fig. 27.4
Scattered lipoblasts with markedly hyperchromatic nuclei and cytologic atypia are seen in lipoblastoma
Fig. 27.5
Adipocytes with multinucleation, microvesiculation, and atypical nuclei are present in lipoblastoma
A related entity is known as lipoblastomatosis, in which multiple lesions with identical histologic features are present [30]. Some authors differentiate lipoblastoma from lipoblastomatosis based upon the latter’s infiltrative growth pattern [26].
Due to the myxoid stroma and lipoblasts, it may be difficult to separate lipoblastoma from myxoid liposarcoma, although cytogenetic studies now make this distinction a straightforward one [28, 31]. Lipomas also enter the differential diagnosis in some cases, but they are separated from lipoblastomas based upon the presence of lipoblasts [27]. Some authors consider lipofibromas to be a sclerosing variant of lipoblastomas, but others argue that based upon different immunostaining properties, lipofibromas are best thought of as discrete entities [32].
27.3.3 Pathogenesis
Lipoblastoma is an adipose tissue tumor that sometimes occurs in children. Chromosomal rearrangement of the 8q11–q13 region is a sensitive (77 %) and specific (98 %) marker for lipoblastoma [33, 34]. PLAG1, located at 8q12.1, has been identified as a target gene in this tumor [35], and FISH analysis for the detection of specific rearrangements of PLAG1 is a sensitive test for lipoblastoma [34]. Translocations or inversions involving PLAG1 in lipoblastoma generate fusions with a variety of other genes, including COL1A2, HAS2, RAD51L1, COL3A1, and RAB2A [34–37]. The fusion of PLAG1 with its partner results in promoter swapping in which the PLAG1 gene is placed under the control of a transcriptionally active promoter, resulting in the ectopic over-expression of PLAG1. PLAG1 is a zinc finger protein that functions as a transcription factor and regulates the expression of key growth factors, such as insulin growth factor II, resulting in dysregulated cell proliferation and tumorigenesis [38, 39].
27.4 Lipoma
27.4.1 Clinical Features
Lipomas are benign mesenchymal tumors of mature adipocytes. They are not commonly seen in children, but they are a common type of soft tissue tumors described in adults [40]. Prevalence is higher in males than in females. No racial predilection exists.
Superficial lipomas are the subtype most commonly seen, and present as variably sized, well-circumscribed, soft, rubbery, skin-colored subcutaneous nodules at the neck, upper torso, abdomen, shoulders, and proximal extremities [40]. These tumors are benign and may be surgically excised if desired.
27.4.2 Histology
Lipoma can occur in the dermis or the subcutis as a well-circumscribed proliferation of mature adipocytes (Fig. 27.6). A thin fibrous capsule encapsulates the tumor. Fibrous septa comprised of collagen-containing blood vessels surround each of the lobules within the lesion. Some lipomas contain foci of fibrosis, giving rise to the term lipofibromas . There are other cases in which smooth muscle or eccrine ducts comprise part of the tumors.
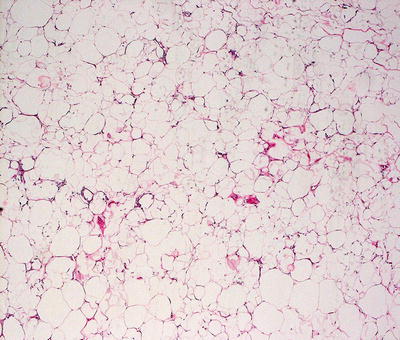
Fig. 27.6
Lipoma is characterized by a well-circumscribed proliferation of mature adipocytes without cytologic atypia or nuclear pleomorphism
27.4.3 Pathogenesis
Most lipomas in children are sporadic. However, some pediatric lipomas occur in syndromic conditions, such as Proteus syndrome , multiple endocrine neoplasia type 1 (MEN1), and Bannayan-Riley-Ruvalcaba syndrome [34, 41–43]. The cytogenetics of lipoma in children is similar to that in adult lipoma. Rearrangements of chromosomal regions 12q14–q15 and 6p21 involving HMGA2 and HMGA1 genes frequently occur in this tumor [34, 44]. So far, six genes have been identified to fuse with HMGA2 in lipoma. The most frequent partner is the lipoma preferred partner (LPP) gene [45]. The other genes are CXCR7, EBF1, LHFP, PPAP2B, and NFIB [34]. It is not known whether some partner genes of HMGA2 may have a specific role in the onset of lipoma. A recent study identified the presence of CD34-positive cells in lipoma around small adipocytes, and showed altered biological activity such as proliferation, apoptosis, and stemness. These findings suggest the involvement of precursor cells in the development of this tumor [46].
27.5 Angiolipoma
27.5.1 Clinical Features
Angiolipomas represent 5–17 % of all lipomas [47]. Lesions are subcategorized into a non-infiltrating variant and a deeper, infiltrating variant with extension into the underlying smooth muscle and soft tissues [47]. Non-infiltrating angiolipomas most often occur in male adolescents and young adults, rarely presenting before puberty.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


