Procedure 90 Total Wrist Arthroplasty
Indications
 Destructive and painful wrist conditions resulting from rheumatoid arthritis (RA), osteoarthritis (OA), or trauma
Destructive and painful wrist conditions resulting from rheumatoid arthritis (RA), osteoarthritis (OA), or trauma
 The procedure is contraindicated in patients with the following conditions:
The procedure is contraindicated in patients with the following conditions:
Examination/Imaging
Clinical Examination






Surgical Anatomy
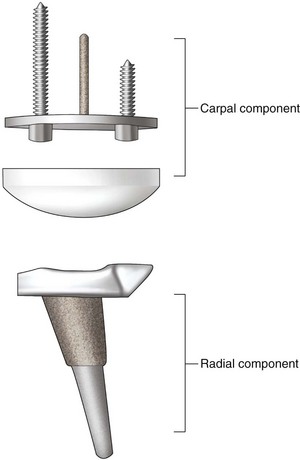
 The implant described in this chapter is the Universal II implant design, which is the most popular total wrist arthroplasty implant used in the United States. Other implant designs are available, but comparative or long-term studies are not presented to determine which implant type is most durable and has the lowest complication rate. The implant design consists of two components. The carpal component is fixated with two screws (Fig. 90-1).
The implant described in this chapter is the Universal II implant design, which is the most popular total wrist arthroplasty implant used in the United States. Other implant designs are available, but comparative or long-term studies are not presented to determine which implant type is most durable and has the lowest complication rate. The implant design consists of two components. The carpal component is fixated with two screws (Fig. 90-1).


 The size of the implant placed can be estimated preoperatively from the wrist radiograph.
The size of the implant placed can be estimated preoperatively from the wrist radiograph.


Exposures
 An 8-cm incision is made on the dorsal wrist, centered on the axis of the long finger metacarpal (Fig. 90-2).
An 8-cm incision is made on the dorsal wrist, centered on the axis of the long finger metacarpal (Fig. 90-2).
 Radial and ulnar skin flaps are elevated, and the extensor retinaculum is visualized.
Radial and ulnar skin flaps are elevated, and the extensor retinaculum is visualized.
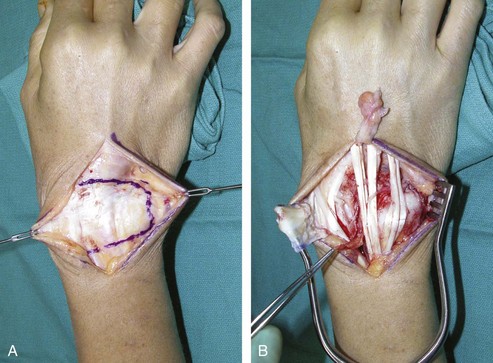
 The entire extensor retinaculum is elevated from the sixth dorsal compartment all the way to the radial attachment over the first compartment. The septa between the compartments are taken down to create a continuous flap of extensor retinaculum. The elevation of the extensor retinaculum stops between the first and second compartments (Fig. 90-3).
The entire extensor retinaculum is elevated from the sixth dorsal compartment all the way to the radial attachment over the first compartment. The septa between the compartments are taken down to create a continuous flap of extensor retinaculum. The elevation of the extensor retinaculum stops between the first and second compartments (Fig. 90-3).
 The extensor tendons are then retracted to expose the wrist.
The extensor tendons are then retracted to expose the wrist.
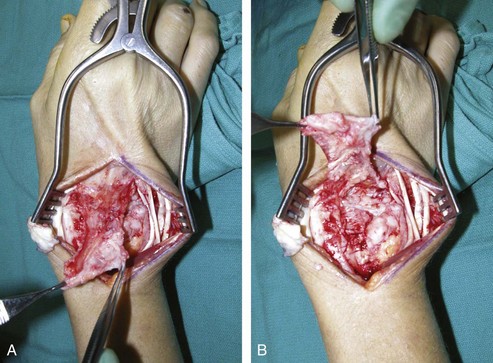
 The wrist capsule is elevated subperiosteally proximal to the radiocarpal joint as a rectangular, distally base flap (Fig. 90-4A and B). The purpose of the wrist capsular flap is to cover and to provide stout capsular support for the implant.
The wrist capsule is elevated subperiosteally proximal to the radiocarpal joint as a rectangular, distally base flap (Fig. 90-4A and B). The purpose of the wrist capsular flap is to cover and to provide stout capsular support for the implant.

Pearls
If there is arthritic change involving the DRU joint, a Darrach procedure is performed by resecting the distal ulna at a 45-degree oblique apex-ulnar angle. RA patients often have DRU disease, and distal ulna excision is performed to alleviate future problems. For OA patients with only radiocarpal disease, the radioulnar joint can be preserved.
The head of the resected ulna should be saved for bone graft.
The ECRB, and preferably the ECRL tendon as well, should be intact or otherwise reconstructible.
A segment of the posterior interosseous nerve can be excised just proximal to the radiocarpal joint.
Procedure
Step 1
 The wrist is flexed to have an end-on view of the radius articular surface. A bone awl is placed 5 mm below the dorsal articular surface of the radius just slightly radial to the Lister tubercle (Fig. 90-5).
The wrist is flexed to have an end-on view of the radius articular surface. A bone awl is placed 5 mm below the dorsal articular surface of the radius just slightly radial to the Lister tubercle (Fig. 90-5).
 The radial alignment guide is inserted into the cavity created by the awl, and fluoroscopy is used to confirm that the guide rod is centered in the radius, both in the anteroposterior and lateral planes (Fig. 90-6).
The radial alignment guide is inserted into the cavity created by the awl, and fluoroscopy is used to confirm that the guide rod is centered in the radius, both in the anteroposterior and lateral planes (Fig. 90-6).
Related posts:
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


