Procedure 88 Four-Corner Fusion Using a Circular Plate
 See Video 66: 4-Corner Fusion with a Circular Plate
See Video 66: 4-Corner Fusion with a Circular Plate



Examination/Imaging
Clinical Examination
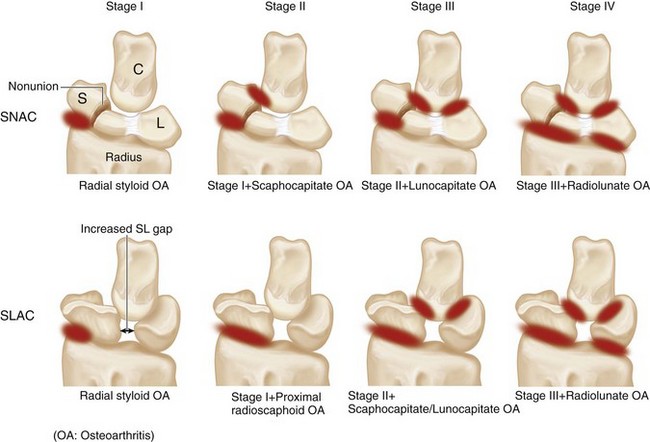
 A sequential progression of arthritic changes has been described for scaphoid nonunion and static scapholunate instability. They are called the scaphoid nonunion advanced collapse (SNAC) and scapholunate advanced collapse (SLAC), respectively (Fig. 88-1).
A sequential progression of arthritic changes has been described for scaphoid nonunion and static scapholunate instability. They are called the scaphoid nonunion advanced collapse (SNAC) and scapholunate advanced collapse (SLAC), respectively (Fig. 88-1).




Imaging
 Standard wrist posteroanterior and lateral views are usually sufficient in SNAC/SLAC wrists. One should be able to determine whether there is arthritis involving the capitate (PRC cannot be done) or arthritis involving the lunate fossa of the radius (both PRC and four-corner fusion cannot be done). If the radiograph shows ulnar translocation of the carpus, it means that the palmar radiocarpal ligaments, especially the radioscaphocapitate, are lax, and a PRC cannot be done.
Standard wrist posteroanterior and lateral views are usually sufficient in SNAC/SLAC wrists. One should be able to determine whether there is arthritis involving the capitate (PRC cannot be done) or arthritis involving the lunate fossa of the radius (both PRC and four-corner fusion cannot be done). If the radiograph shows ulnar translocation of the carpus, it means that the palmar radiocarpal ligaments, especially the radioscaphocapitate, are lax, and a PRC cannot be done.

Surgical Anatomy
 The distal radius has two articular fossae for the scaphoid and lunate. The scaphoid fossa is shaped like a spoon and narrows as it approaches the radial styloid. This results in incongruency between the scaphoid and the scaphoid fossa during positional changes and results in uneven loading of scaphoid fossa, making degenerative changes of the radioscaphoid joint common. On the other hand, the lunate fossa is spherical and remains congruently loaded in all positions of the lunate, making the radiolunate joint highly resistant to degenerative changes.
The distal radius has two articular fossae for the scaphoid and lunate. The scaphoid fossa is shaped like a spoon and narrows as it approaches the radial styloid. This results in incongruency between the scaphoid and the scaphoid fossa during positional changes and results in uneven loading of scaphoid fossa, making degenerative changes of the radioscaphoid joint common. On the other hand, the lunate fossa is spherical and remains congruently loaded in all positions of the lunate, making the radiolunate joint highly resistant to degenerative changes.
Exposures
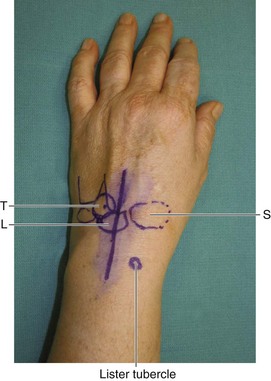
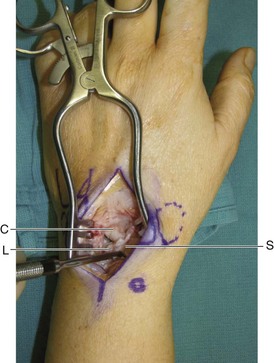
 A 6-cm dorsal longitudinal incision centered over the radiocarpal joint in line with the long finger metacarpal is made (Fig. 88-2). Sharp dissection is carried down to the extensor retinaculum. Skin and subcutaneous tissue flaps are raised on both sides. The third dorsal compartment is identified and opened along its entire length. The extensor pollicis longus (EPL) tendon is left in its sheath and not transposed. One must know the location of the EPL when incising the wrist capsule proximally. The wrist capsule is opened longitudinally and dissection performed to elevate the second and fourth compartments such that the second and fourth compartment tendons are maintained within the compartment. This exposes the scaphoid, lunate, triquetrum, capitate, and hamate.
A 6-cm dorsal longitudinal incision centered over the radiocarpal joint in line with the long finger metacarpal is made (Fig. 88-2). Sharp dissection is carried down to the extensor retinaculum. Skin and subcutaneous tissue flaps are raised on both sides. The third dorsal compartment is identified and opened along its entire length. The extensor pollicis longus (EPL) tendon is left in its sheath and not transposed. One must know the location of the EPL when incising the wrist capsule proximally. The wrist capsule is opened longitudinally and dissection performed to elevate the second and fourth compartments such that the second and fourth compartment tendons are maintained within the compartment. This exposes the scaphoid, lunate, triquetrum, capitate, and hamate.
 Figure 88-3 shows a Freer elevator within the SL interval demonstrating a complete rupture of the SL ligament.
Figure 88-3 shows a Freer elevator within the SL interval demonstrating a complete rupture of the SL ligament.
Procedure
Step 1: Scaphoidectomy
 The scapholunate ligament is divided, and a sharp-edged Freer or an Obwegeser periosteal elevator is used to separate the scaphoid from the volar capsule. After adequate detachment of the volar capsule, a rongeur is used to hold the scaphoid and using a twisting motion, the surgeon removes the scaphoid as one piece.
The scapholunate ligament is divided, and a sharp-edged Freer or an Obwegeser periosteal elevator is used to separate the scaphoid from the volar capsule. After adequate detachment of the volar capsule, a rongeur is used to hold the scaphoid and using a twisting motion, the surgeon removes the scaphoid as one piece.
 The cancellous bone within the scaphoid is harvested for bone grafting.
The cancellous bone within the scaphoid is harvested for bone grafting.
Step 1 Pearls
A 0.062-inch K-wire inserted into the scaphoid to serve as a joystick can make dissection of the scaphoid from the volar capsule easier.
The entire scaphoid is removed in one piece and not in a piecemeal fashion. This ensures that portions of the scaphoid attached to the volar capsule are not left behind.





