Procedure 82 Radioulnar Ligament Reconstruction for Chronic Distal Radioulnar Joint Instability
 See Video 60: Reconstruction for Chronic Volar Subluxation of the Ulna
See Video 60: Reconstruction for Chronic Volar Subluxation of the Ulna
See Video 61: Distal Radioulnar Joint Ligament Reconstruction for Ligamentous Instability

Examination/Imaging
Clinical Examination
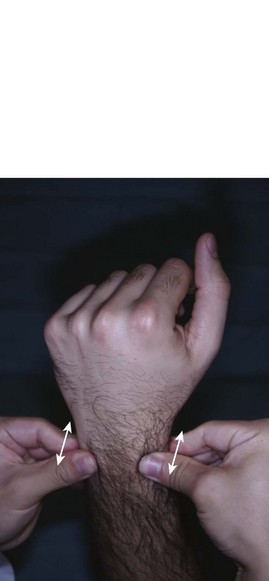
 DRU joint instability may coexist with other causes of ulnar-sided wrist pain. These include extensor carpi ulnaris (ECU) tendinitis, flexor carpi ulnaris (FCU) tendonitis, ECU subluxation, ulnar impaction syndrome, lunotriquetral (LT) instability, and pisotriquetral arthritis. It is important to consider these conditions before attributing the symptoms to DRU joint instability. The following clinical tests are suggestive of DRU joint instability:
DRU joint instability may coexist with other causes of ulnar-sided wrist pain. These include extensor carpi ulnaris (ECU) tendinitis, flexor carpi ulnaris (FCU) tendonitis, ECU subluxation, ulnar impaction syndrome, lunotriquetral (LT) instability, and pisotriquetral arthritis. It is important to consider these conditions before attributing the symptoms to DRU joint instability. The following clinical tests are suggestive of DRU joint instability:




Imaging
 A posteroanterior view radiograph may show widening of the DRU joint, and the lateral view demonstrates the ulnar head dorsal or volar to the radius (Fig. 82-4). A weighted lateral view (taken with patient holding 5 to 8 pounds of weight) can be used to demonstrate the instability that occurs only on loading (Fig. 82-5). Other indirect signs of instability include a basal ulnar styloid fracture (Fig. 82-6) and a displaced fleck fracture from the fovea.
A posteroanterior view radiograph may show widening of the DRU joint, and the lateral view demonstrates the ulnar head dorsal or volar to the radius (Fig. 82-4). A weighted lateral view (taken with patient holding 5 to 8 pounds of weight) can be used to demonstrate the instability that occurs only on loading (Fig. 82-5). Other indirect signs of instability include a basal ulnar styloid fracture (Fig. 82-6) and a displaced fleck fracture from the fovea.

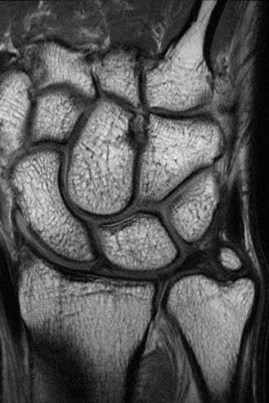
 Magnetic resonance imaging (Fig. 82-7) and arthroscopy are useful in assessment of the triangular fibrocartilage complex (TFCC) and in ruling out other causes of ulnar-sided wrist pain.
Magnetic resonance imaging (Fig. 82-7) and arthroscopy are useful in assessment of the triangular fibrocartilage complex (TFCC) and in ruling out other causes of ulnar-sided wrist pain.



Pearls
To ensure that the lateral radiograph is adequate, the index, long, and ring metacarpals; the proximal pole of the scaphoid on the lunate; and the radial styloid in the center of the lunate should all be superimposed on one another. Additionally, the palmar surface of the pisiform should be visible midway between the palmar surfaces of the distal pole of the scaphoid and the capitate (Fig. 82-8).

Surgical Anatomy
 The DRU joint is formed by the sigmoid notch of the radius and the ulnar head. It is the distal pivot for pronosupination. This joint is stabilized predominantly by ligaments, the fibrocartilaginous lips at the rim of the sigmoid notch, and the shape of the sigmoid notch in the coronal plane.
The DRU joint is formed by the sigmoid notch of the radius and the ulnar head. It is the distal pivot for pronosupination. This joint is stabilized predominantly by ligaments, the fibrocartilaginous lips at the rim of the sigmoid notch, and the shape of the sigmoid notch in the coronal plane.
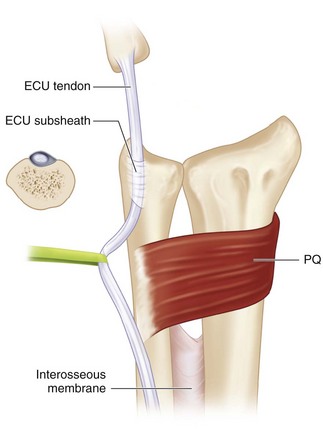
 The stabilizers of the DRU joint include the TFCC, pronator quadratus (PQ), ECU, and interosseous membrane (Fig. 82-9).
The stabilizers of the DRU joint include the TFCC, pronator quadratus (PQ), ECU, and interosseous membrane (Fig. 82-9).

 The palmar and dorsal radiolulnar ligaments are the main stabilizers of the DRU joint. These ligaments extend from the palmar and dorsal distal margins of the sigmoid notch and converge in a triangular configuration to attach to the ulna. Each radioulnar ligament divides in the coronal plane into a deep limb that inserts into the fovea and a superficial limb that inserts into the midportion of the ulnar styloid (Fig. 82-10).
The palmar and dorsal radiolulnar ligaments are the main stabilizers of the DRU joint. These ligaments extend from the palmar and dorsal distal margins of the sigmoid notch and converge in a triangular configuration to attach to the ulna. Each radioulnar ligament divides in the coronal plane into a deep limb that inserts into the fovea and a superficial limb that inserts into the midportion of the ulnar styloid (Fig. 82-10).
Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


