Procedure 80 Corrective Osteotomy of Malunited Distal Radius Fractures
Indications
 Deformity by itself may or may not be symptomatic. A decision for surgery should be based on functional impairment, pain, loss of motion, and limitation of grip strength.
Deformity by itself may or may not be symptomatic. A decision for surgery should be based on functional impairment, pain, loss of motion, and limitation of grip strength.
 Alteration of radiocarpal alignment will affect normal carpal kinematics and changes in the vectors of the extensor and flexor tendons (Fig. 80-1).
Alteration of radiocarpal alignment will affect normal carpal kinematics and changes in the vectors of the extensor and flexor tendons (Fig. 80-1).
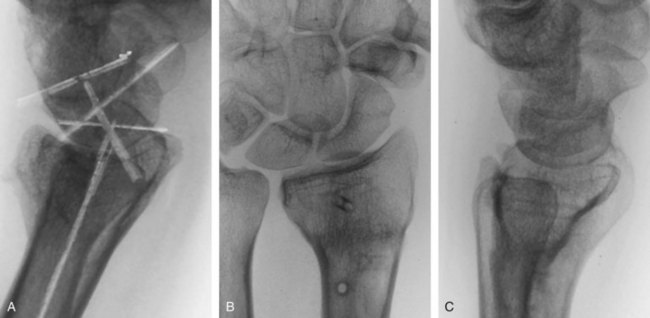
 Dorsally malunited fracture can result in a midcarpal instability (Figs. 80-2 and 80-3).
Dorsally malunited fracture can result in a midcarpal instability (Figs. 80-2 and 80-3).











Examination/Imaging

Imaging
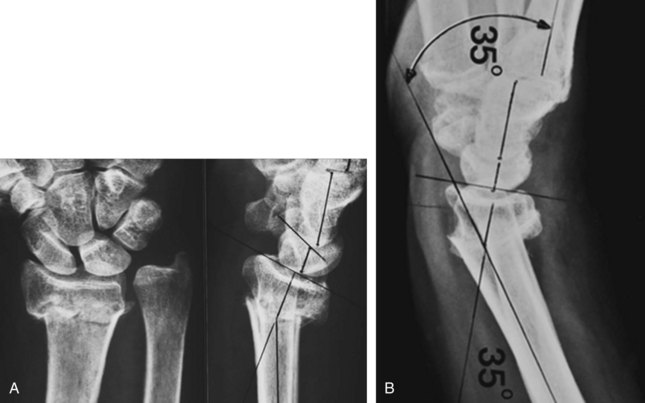
 Standard anteroposterior, lateral, and oblique radiographs of both wrists are essential for preoperative planning.
Standard anteroposterior, lateral, and oblique radiographs of both wrists are essential for preoperative planning.
 For most deformities, tracings can be made from the anteroposterior and lateral radiographs and superimposed on each other. The angle and precise location of the deformity can be identified in the frontal and sagittal planes (Fig. 80-4).
For most deformities, tracings can be made from the anteroposterior and lateral radiographs and superimposed on each other. The angle and precise location of the deformity can be identified in the frontal and sagittal planes (Fig. 80-4).
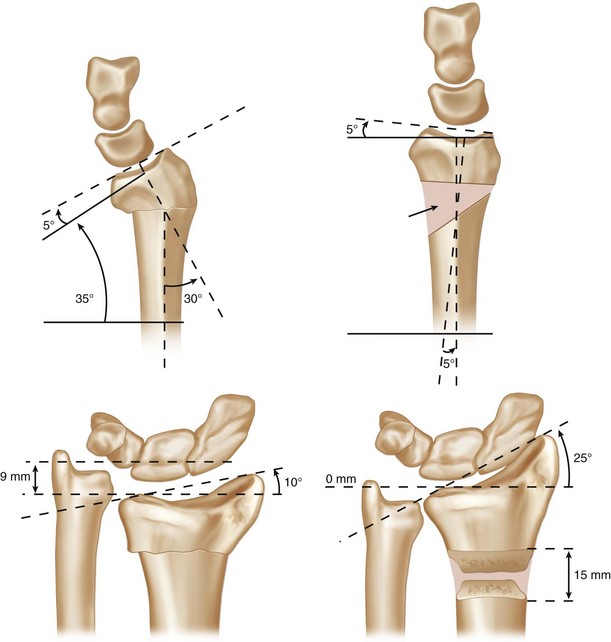
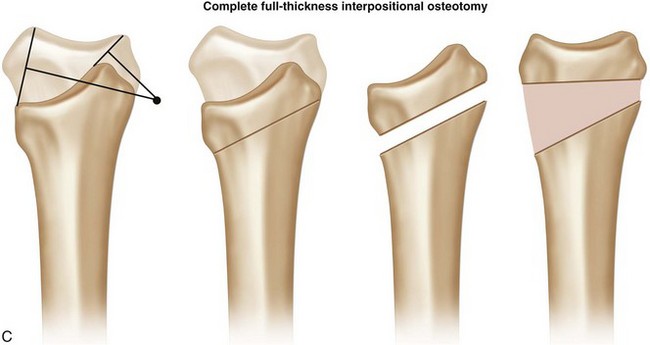
 By superimposing the tracings in the sagittal and frontal planes and drawing a line from the most volar and dorsal lips, a perpendicular line can be drawn midpoint on each line. Where these two intersect will define the type of osteotomy required and the need for lengthening of the distal fragment (Fig. 80-5).
By superimposing the tracings in the sagittal and frontal planes and drawing a line from the most volar and dorsal lips, a perpendicular line can be drawn midpoint on each line. Where these two intersect will define the type of osteotomy required and the need for lengthening of the distal fragment (Fig. 80-5).







Exposures
Volar
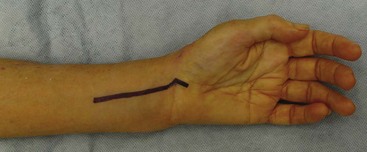
 The distal part of the anterior Henry approach involves exposure between the flexor carpi radialis and radial artery (Fig. 80-6).
The distal part of the anterior Henry approach involves exposure between the flexor carpi radialis and radial artery (Fig. 80-6).
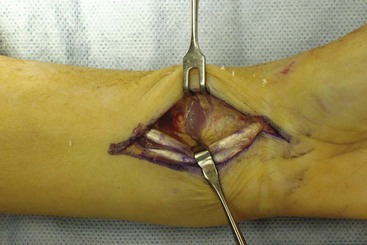
 The muscle belly of the flexor pollicis longus is retracted ulnarly to expose the pronator quadratus, which is elevated from its insertion on the radius (Fig. 80-7).
The muscle belly of the flexor pollicis longus is retracted ulnarly to expose the pronator quadratus, which is elevated from its insertion on the radius (Fig. 80-7).

 Small Hohmann retractors are placed along the borders of the distal radius at the site of the deformity (Fig. 80-8).
Small Hohmann retractors are placed along the borders of the distal radius at the site of the deformity (Fig. 80-8).

Dorsal
 The skin incision is between 6 and 8 cm extending 2 to 3 cm distal to the Lister tubercle (Fig. 80-9).
The skin incision is between 6 and 8 cm extending 2 to 3 cm distal to the Lister tubercle (Fig. 80-9).

Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


