Procedure 8 Acute Repair of Zone 2 Flexor Tendon Injury
 See Video 5: Acute Repair of Zone 2 Flexor Tendon Injury
See Video 5: Acute Repair of Zone 2 Flexor Tendon Injury
Figure 8-7 is adapted from Tang JB. Flexor tendon repair in zone 2C. J Hand Surg [Br]. 1994;19:72-75, with permission from Elsevier. Figure 8-18 is adapted from Strickland JW. Development of flexor tendon surgery: twenty-five years of progress. J Hand Surg [Am]. 2000;25:214-235, with permission from Elsevier.
Indications


Examination/Imaging
Clinical Examination
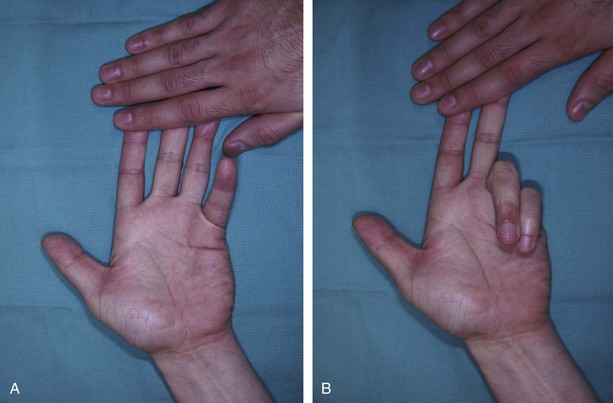
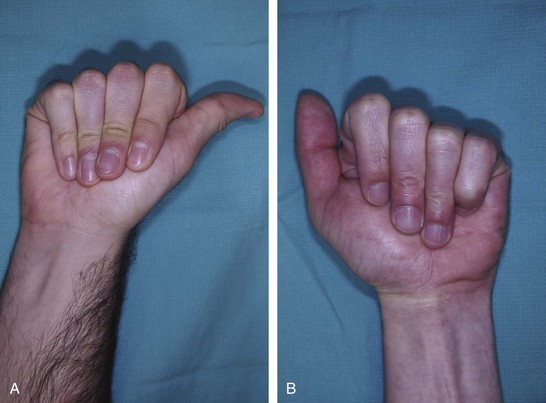
 Patients present with loss of active distal interphalangeal (DIP) and proximal interphalangeal (PIP) joint flexion if both FDP and FDS are divided, or loss of only DIP joint flexion if only FDP has been injured. On inspection, the normal finger cascade is lost with the affected digit in an extended position.
Patients present with loss of active distal interphalangeal (DIP) and proximal interphalangeal (PIP) joint flexion if both FDP and FDS are divided, or loss of only DIP joint flexion if only FDP has been injured. On inspection, the normal finger cascade is lost with the affected digit in an extended position.



 In patients who cannot cooperate (e.g., children or comatose or intoxicated patients), one can look for passive movement of the fingers resulting from the wrist tenodesis effect or by squeezing the forearm muscles (Fig. 8-5). The same maneuvers can be used when trying to differentiate between tendon injury and inability to move as a result of nerve palsy.
In patients who cannot cooperate (e.g., children or comatose or intoxicated patients), one can look for passive movement of the fingers resulting from the wrist tenodesis effect or by squeezing the forearm muscles (Fig. 8-5). The same maneuvers can be used when trying to differentiate between tendon injury and inability to move as a result of nerve palsy.




Imaging
 Preoperative imaging studies are not typically necessary, but anteroposterior and lateral x-rays may help identify associated bony injury. When a patient presents with unstable or intra-articular fractures, rigid fixation of the fracture is performed so that judicious tendon mobilization can be performed after tendon repair.
Preoperative imaging studies are not typically necessary, but anteroposterior and lateral x-rays may help identify associated bony injury. When a patient presents with unstable or intra-articular fractures, rigid fixation of the fracture is performed so that judicious tendon mobilization can be performed after tendon repair.
Surgical Anatomy
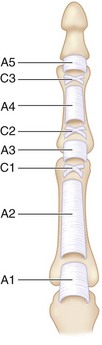
 Zone 2 contains both the FDS and FDP tendons and extends from the proximal edge of the A1 pulley in the palm to the insertion of the FDS over the middle phalanx. It includes four annular pulleys (A1, A2, A3, and A4) and two cruciate pulleys (C1 and C2) (Fig. 8-6).
Zone 2 contains both the FDS and FDP tendons and extends from the proximal edge of the A1 pulley in the palm to the insertion of the FDS over the middle phalanx. It includes four annular pulleys (A1, A2, A3, and A4) and two cruciate pulleys (C1 and C2) (Fig. 8-6).
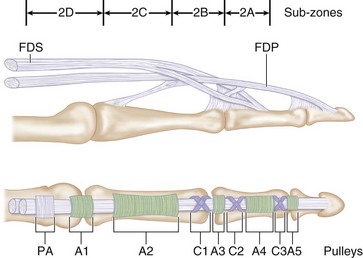
 Zone 2 was subdivided by Tang (1994) into four subzones (Fig. 8-7).
Zone 2 was subdivided by Tang (1994) into four subzones (Fig. 8-7).



Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


