Figure 28.1
H&E 100× paracoccidiomycosis, a dense infiltrate of histocytes
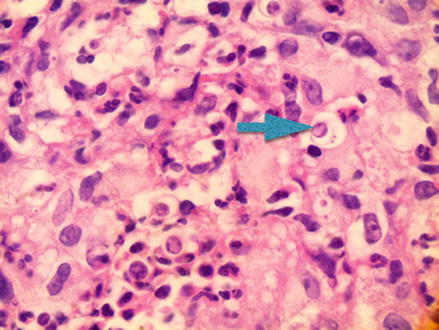
Figure 28.2
H&E 1,000×, note central yeast-like organisms with small daughter yeasts at the peripheral rim
Serological tests are available but not used as they are rarely diagnostic. HIV testing may be performed in patients suspected of infection. Chest radiography should always be performed to check for pulmonary involvement.
Treatment
The first line treatment for moderate cases of infection is itraconazole 100 mg daily for 6 months If that therapy fails, ketoconazole 400 mg daily for 6–18 months may be used. In severe cases of infection or in cases with meningeal involvement, IV amphotericin B 0.4–0.5 mg/kg is recommended daily until a total dose of 1.5–2.5 mg/kg has been administered.
Prevention
When traveling, it is recommended that endemic regions be avoided. Disease presentation can be delayed with cases reported 60 days after initial infection. Early detection and diagnosis is important to prevent disseminated disease, permanent disfigurement and death. Whenever the combination of pulmonary, cutaneous, mucosal, and lymphatic involvement is observed, paracoccidioidomycosis should be at the top of the differential diagnoses list.
Recommended Reading
Related posts:
 6 Year Old White Male with Recurrent Brownish Patches Around Mouth
6 Year Old White Male with Recurrent Brownish Patches Around Mouth
 37 Year Old White Male with Multiple, Brown, Purple Nodules on Arms and Legs
37 Year Old White Male with Multiple, Brown, Purple Nodules on Arms and Legs
 70 Year Old White Male with Grouped Blisters on Right Lower Leg
70 Year Old White Male with Grouped Blisters on Right Lower Leg
 7 Year Old Male with an Enlarging, Round Area of Hair Loss
7 Year Old Male with an Enlarging, Round Area of Hair Loss
 57 Year Old Male with Multiple Widespread Excoriations
57 Year Old Male with Multiple Widespread Excoriations
 46 Year Old Female with Multiple Slightly Eroded Reddish Papules on Her Arm
46 Year Old Female with Multiple Slightly Eroded Reddish Papules on Her Arm
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


