Procedure 78 Dorsal Plate Fixation and Dorsal Distraction (Bridge) Plating for Distal Radius Fractures
Dorsal Plating of Distal Radius Fractures




Examination/Imaging
Clinical Examination
 Initial examination is usually performed in the emergency department and needs to include mechanism and time of injury, hand dominance, medical comorbidities that may alter treatment, and occupation.
Initial examination is usually performed in the emergency department and needs to include mechanism and time of injury, hand dominance, medical comorbidities that may alter treatment, and occupation.
 Assess whether the fracture is an open or closed injury.
Assess whether the fracture is an open or closed injury.

 Identify any associated neurovascular and soft tissue injuries.
Identify any associated neurovascular and soft tissue injuries.
 Identify whether patient has any sign or symptoms of acute median or ulnar nerve injury.
Identify whether patient has any sign or symptoms of acute median or ulnar nerve injury.
Imaging
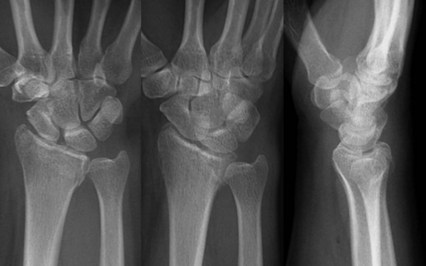
 Initial radiographic evaluation must include posteroanterior, lateral, and oblique views (Fig. 78-1).
Initial radiographic evaluation must include posteroanterior, lateral, and oblique views (Fig. 78-1).



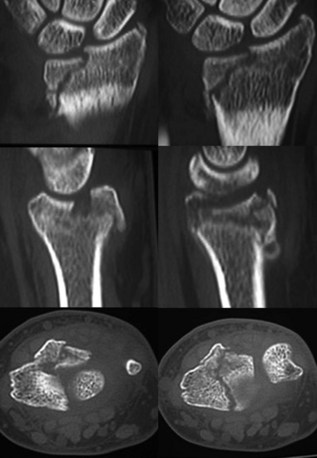
 Computed tomography scan provides excellent delineation of intra-articular extension as well as characterization of fracture comminution for preoperative planning (Fig. 78-2).
Computed tomography scan provides excellent delineation of intra-articular extension as well as characterization of fracture comminution for preoperative planning (Fig. 78-2).

 Proximal injuries must be ruled out by physical examination and radiographs of the elbow.
Proximal injuries must be ruled out by physical examination and radiographs of the elbow.
Surgical Anatomy
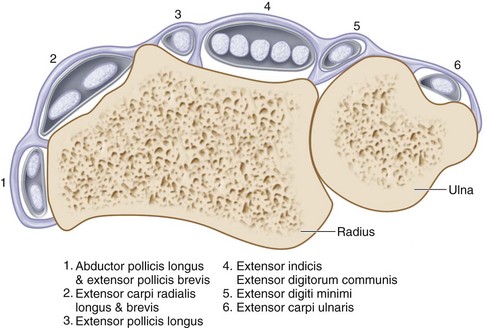
 Knowledge of the anatomic relationships of the extensor retinaculum, six dorsal extensor compartments, and convex dorsoradial cortex is essential for understanding surgical approaches as well as placement of implants on the dorsum of the radius (Fig. 78-3).
Knowledge of the anatomic relationships of the extensor retinaculum, six dorsal extensor compartments, and convex dorsoradial cortex is essential for understanding surgical approaches as well as placement of implants on the dorsum of the radius (Fig. 78-3).






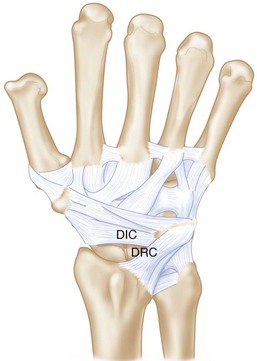
 There are two dorsal ligaments that are intimately associated with the dorsal capsule: the dorsal radiocarpal (DRC) (radiotriquetral) and dorsal intercarpal (DIC) (scaphotriquetral) ligaments (Fig. 78-4).
There are two dorsal ligaments that are intimately associated with the dorsal capsule: the dorsal radiocarpal (DRC) (radiotriquetral) and dorsal intercarpal (DIC) (scaphotriquetral) ligaments (Fig. 78-4).
Exposures
 The dorsal distal radius is approached through a straight, longitudinal incision in line with the third metacarpal and centered just ulnar to the Lister tubercle, between the third and fourth dorsal compartments (Fig. 78-5).
The dorsal distal radius is approached through a straight, longitudinal incision in line with the third metacarpal and centered just ulnar to the Lister tubercle, between the third and fourth dorsal compartments (Fig. 78-5).
 Care is taken to identify and avoid injury to the superficial branch of the radial nerve.
Care is taken to identify and avoid injury to the superficial branch of the radial nerve.

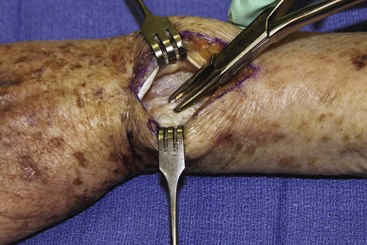
 The third dorsal compartment is longitudinally incised to mobilize the EPL tendon (Fig. 78-6).
The third dorsal compartment is longitudinally incised to mobilize the EPL tendon (Fig. 78-6).


 The distal radius is exposed sharply by elevation of the periosteum.
The distal radius is exposed sharply by elevation of the periosteum.




Pearls
Large, longitudinal veins should be preserved if possible, but crossing veins may be divided.
Full-thickness flaps will contain the dorsal sensory branches of the ulnar and radial nerve and protect them.
Subperiosteal elevation of the fourth compartment minimizes implant contact with the extensor tendons.
Pitfalls
If the distal extension of the incision is past the base of the third metacarpal, the dorsal sensory branches of both the radial and ulnar nerves are at risk.
The EPL tendon is left above the retinaculum at closure to minimize the risk for tendon injury by ischemia or direct contact with an implant.
Care must be exercised not to enter the DRUJ. If the dorsal radioulnar ligament is divided during ulnar dissection, radioulnar instability can result.
The intercarpal ligaments must be protected during capsulotomy.
Procedure
Dorsal Plate Fixation for Distal Radius Fractures
Step 1: Reduction of Dorsally Angulated Fractures
 Once the proximal fracture lines and articular surface are exposed and assessed, all hematoma is evacuated.
Once the proximal fracture lines and articular surface are exposed and assessed, all hematoma is evacuated.
 Lister tubercle is removed with a rongeur or small osteotome (Fig. 78-7).
Lister tubercle is removed with a rongeur or small osteotome (Fig. 78-7).



Step 2: Fixation of Dorsally Angulated Fractures
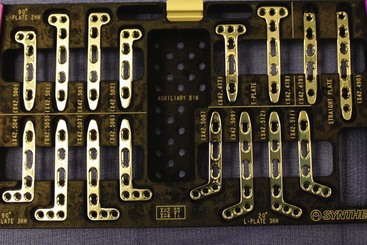
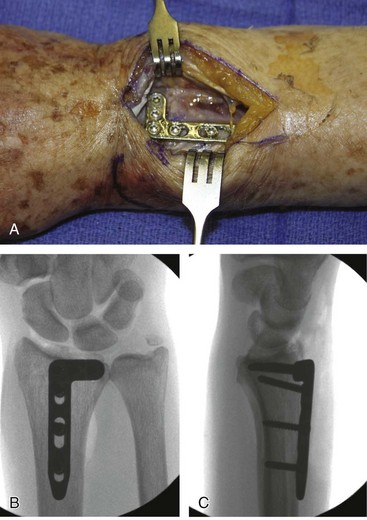
 After satisfactory reduction is performed, a 2.4-mm low-profile dorsal T-plate (Fig. 78-8) can be placed directly over the dorsal surface of the distal radius.
After satisfactory reduction is performed, a 2.4-mm low-profile dorsal T-plate (Fig. 78-8) can be placed directly over the dorsal surface of the distal radius.






Step 3: Reduction and Fixation of Dorsal Marginal Fractures
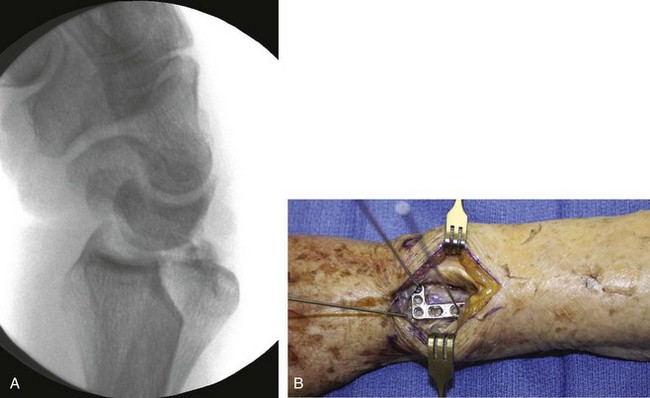
 It is important to assess carpal subluxation and initially restore the radial styloid fragment if present (Fig. 78-9A).
It is important to assess carpal subluxation and initially restore the radial styloid fragment if present (Fig. 78-9A).
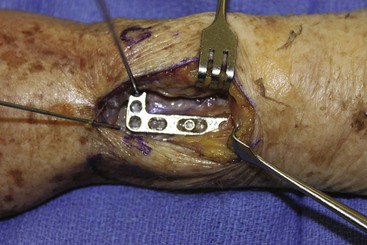
 This reduction is usually accomplished with traction and ulnar deviation of the hand and wrist, and then provisional K-wire fixation (Figs. 78-9B and 78-10).
This reduction is usually accomplished with traction and ulnar deviation of the hand and wrist, and then provisional K-wire fixation (Figs. 78-9B and 78-10).

 Preliminary fixation of the plate with a single, bicortical screw placed in the oblong hole will allow for proximal-distal plate adjustments as determined clinically and fluoroscopically (Fig. 78-11).
Preliminary fixation of the plate with a single, bicortical screw placed in the oblong hole will allow for proximal-distal plate adjustments as determined clinically and fluoroscopically (Fig. 78-11).




 If the plate is acting purely as a buttress, distal locking screws are not necessary.
If the plate is acting purely as a buttress, distal locking screws are not necessary.

 One or two additional bicortical screws are placed proximally to the proximal extent of the fracture to finalize construct (Figure 78-12).
One or two additional bicortical screws are placed proximally to the proximal extent of the fracture to finalize construct (Figure 78-12).

Step 3 Pitfalls
Failure to recognize styloid component or any volar-ulnar fragments will lead to incongruity of articular surface and radiocarpal arthrosis.
Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


