Procedure 77 Volar Plating of Distal Radius Fractures
 See Video 58: Volar Locking Plate Fixation for Distal Radius Fractures
See Video 58: Volar Locking Plate Fixation for Distal Radius Fractures









Surgical Anatomy
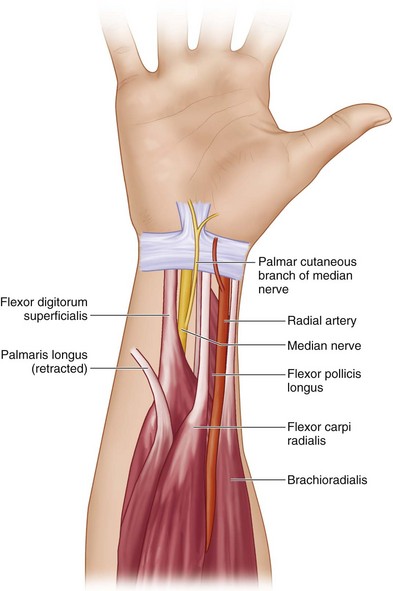
 Drawing of volar anatomy of forearm and wrist. The surgical interval is between the flexor carpi radialis (FCR) tendon and radial artery and brachioradialis (BR) insertion (Fig. 77-2).
Drawing of volar anatomy of forearm and wrist. The surgical interval is between the flexor carpi radialis (FCR) tendon and radial artery and brachioradialis (BR) insertion (Fig. 77-2).





Exposures
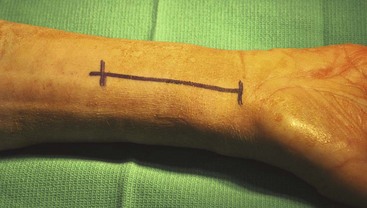
 An incision about 7 cm in length is made over the forearm between the radial artery and the FCR. The distal aspect of the incision stops at the volar wrist crease (Fig. 77-3). If the incision needs to be extended more distally, a V-shaped zigzag extension should be made.
An incision about 7 cm in length is made over the forearm between the radial artery and the FCR. The distal aspect of the incision stops at the volar wrist crease (Fig. 77-3). If the incision needs to be extended more distally, a V-shaped zigzag extension should be made.
 The FCR tendon is exposed and released from its sheath. The dissection should remain on the radial aspect of the FCR (Fig. 77-4).
The FCR tendon is exposed and released from its sheath. The dissection should remain on the radial aspect of the FCR (Fig. 77-4).
 The radial artery and its accompanying venae comitantes are exposed and retracted radially. All ulnar crossing vessels are coagulated (Fig. 77-5).
The radial artery and its accompanying venae comitantes are exposed and retracted radially. All ulnar crossing vessels are coagulated (Fig. 77-5).
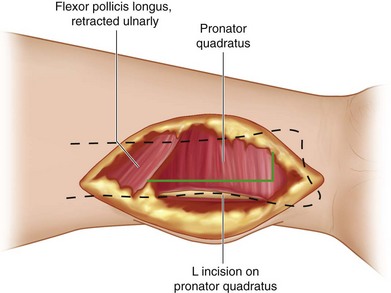
 The PQ is elevated from the distal radius by making an L-shaped incision and releasing it radially and distally (Fig. 77-6). The PQ is sharply released from the radius to expose the fracture (Fig. 77-7).
The PQ is elevated from the distal radius by making an L-shaped incision and releasing it radially and distally (Fig. 77-6). The PQ is sharply released from the radius to expose the fracture (Fig. 77-7).



Pearls
It is helpful to mobilize the radial artery and ligate its small crossing branches during the exposure. This minimizes bleeding and also allows for better exposure of the BR for release.
Do not take the reflection of the soft tissue too far distally on the radius. This may result in release of the volar carpal ligaments from the distal radius and induce carpal instability.
Procedure
Step 1
 The volar radius is exposed, and the distal fragment is exposed by releasing the BR tendon. The distal fragment is usually displaced dorsally (Fig. 77-8).
The volar radius is exposed, and the distal fragment is exposed by releasing the BR tendon. The distal fragment is usually displaced dorsally (Fig. 77-8).
 A Freer elevator may be used to lever the distal fragment for fracture reduction (Fig. 77-9). The elevator should be inserted to the dorsal cortex to completely disimpact the distal fragment to aid in reduction.
A Freer elevator may be used to lever the distal fragment for fracture reduction (Fig. 77-9). The elevator should be inserted to the dorsal cortex to completely disimpact the distal fragment to aid in reduction.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


