Procedure 75 Scaphotrapeziotrapezoid Arthrodesis and Lunate Excision with Replacement by Palmaris Longus Tendon
Indications




Examination/Imaging
Clinical Examination





Imaging
Plain Radiographs
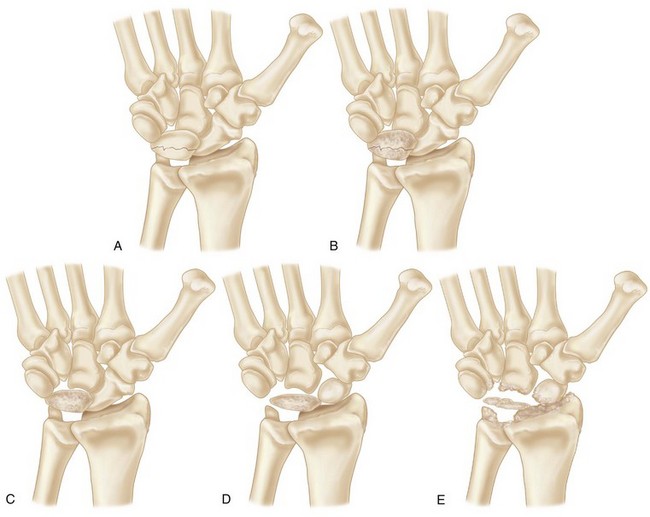
 Staging: Lichtman modification of Stahl staging
Staging: Lichtman modification of Stahl staging
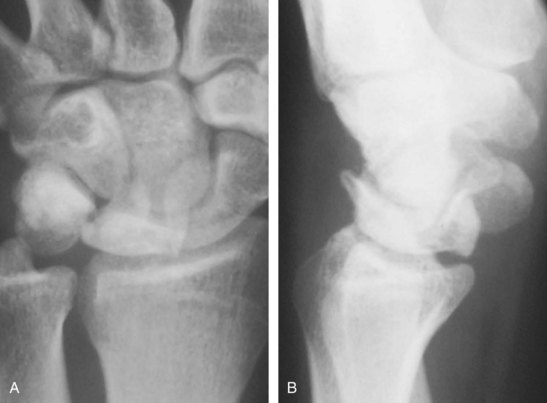
 Posteroanterior (PA) and lateral radiographs with the wrist in neutral rotation and neutral flexion-extension (Fig. 75-2).
Posteroanterior (PA) and lateral radiographs with the wrist in neutral rotation and neutral flexion-extension (Fig. 75-2).

 Lunate sclerosis, carpal instability patterns, and fragmentation are seen.
Lunate sclerosis, carpal instability patterns, and fragmentation are seen.

 Evaluation of relationship among scaphoid, trapezium, and trapezoid.
Evaluation of relationship among scaphoid, trapezium, and trapezoid.
Computed Tomography
 Computed tomography (CT) is needed to evaluate precisely the bony architecture of the lunate and the remainder of the carpus to determine which procedure is indicated and to determine whether arthritic changes of the midcarpal and radiocarpal joints are present.
Computed tomography (CT) is needed to evaluate precisely the bony architecture of the lunate and the remainder of the carpus to determine which procedure is indicated and to determine whether arthritic changes of the midcarpal and radiocarpal joints are present.
 A CT scan is useful for evaluation of fragmentation or fracture patterns and associated collapse.
A CT scan is useful for evaluation of fragmentation or fracture patterns and associated collapse.
Magnetic Resonance Imaging
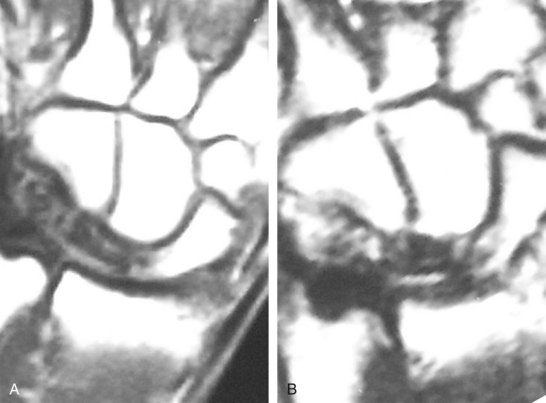
 MRI will show decreased uptake in both T1- and T2-weighted images. Gadolinium contrast has improved diagnosis and evaluation of lunate vascularity (Fig. 75-3).
MRI will show decreased uptake in both T1- and T2-weighted images. Gadolinium contrast has improved diagnosis and evaluation of lunate vascularity (Fig. 75-3).
 It is important to differentiate between ulnar impaction of the lunate and true Kienböck disease.
It is important to differentiate between ulnar impaction of the lunate and true Kienböck disease.


Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


