Procedure 74 Lunotriquetral Ligament Reconstruction Using a Slip of the Extensor Carpi Ulnaris Tendon
 See Video 55: Lunotriquetral Ligament Reconstruction Using the Extensor Carpi Ulnaris Tendon
See Video 55: Lunotriquetral Ligament Reconstruction Using the Extensor Carpi Ulnaris Tendon

Examination/Imaging
Clinical Examination
 Patients with LT instability present with ulnar-sided wrist pain. Other causes of ulnar-sided wrist pain include ulnar impaction syndrome, extensor carpi ulnaris (ECU) subluxation, distal radioulnar joint (DRUJ) instability, triangular fibrocartilage complex (TFCC) injuries, pisotriquetral arthritis, and hook of hamate fractures.
Patients with LT instability present with ulnar-sided wrist pain. Other causes of ulnar-sided wrist pain include ulnar impaction syndrome, extensor carpi ulnaris (ECU) subluxation, distal radioulnar joint (DRUJ) instability, triangular fibrocartilage complex (TFCC) injuries, pisotriquetral arthritis, and hook of hamate fractures.



Imaging
 A posteroanterior radiograph may show a step-off between the lunate and triquetrum and the disruption of the normal convex arc of the proximal carpal row (Gilula line). Unlike the scapholunate dissociation, a gap in the LT interval is rarely seen in patients with LT instability.
A posteroanterior radiograph may show a step-off between the lunate and triquetrum and the disruption of the normal convex arc of the proximal carpal row (Gilula line). Unlike the scapholunate dissociation, a gap in the LT interval is rarely seen in patients with LT instability.
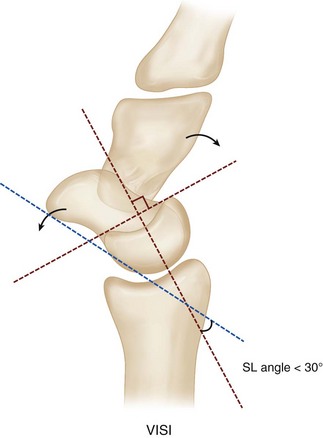
 Plain radiographs may show a volar intercalated segment instability (VISI) deformity, marked by volar tilting of the lunate (Fig. 74-3).
Plain radiographs may show a volar intercalated segment instability (VISI) deformity, marked by volar tilting of the lunate (Fig. 74-3).
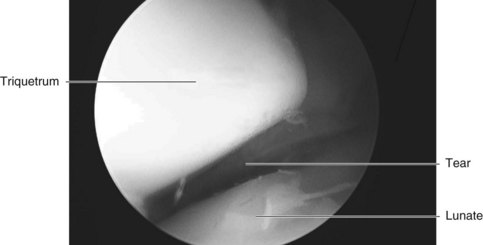
 Wrist arthroscopy is useful to diagnose an LT ligament tear when plain radiographs are normal (Fig. 74-4). The LT interosseous space is tightly closed in normal subjects, whereas in LT dissociations, the space can be opened with the probe, and a gap can be seen between the involved carpals from the midcarpal portal.
Wrist arthroscopy is useful to diagnose an LT ligament tear when plain radiographs are normal (Fig. 74-4). The LT interosseous space is tightly closed in normal subjects, whereas in LT dissociations, the space can be opened with the probe, and a gap can be seen between the involved carpals from the midcarpal portal.
Surgical Anatomy
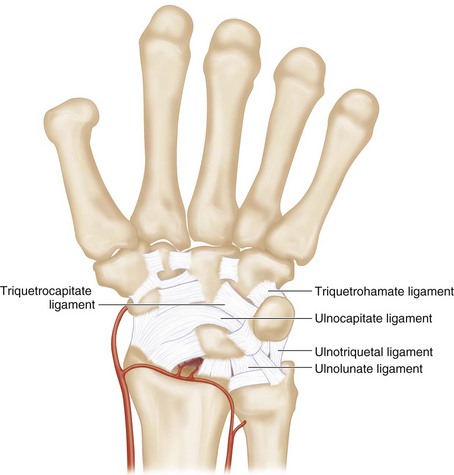
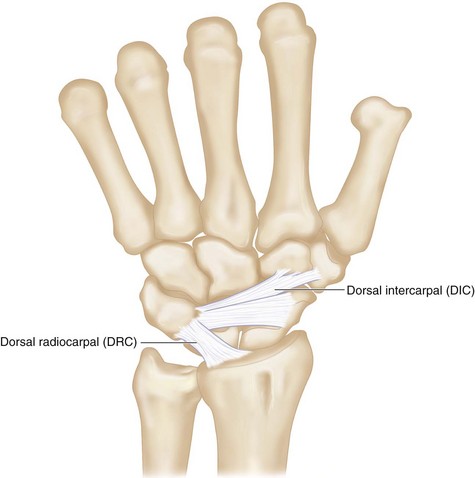
 The LT ligament is C shaped, spanning the (1) dorsal, (2) proximal, and (3) palmar edges of the joint surfaces. The palmar region is the thickest and strongest. It is the primary stabilizer of the LT joint. Additional supports of the LT joint include the ulnocarpal (ulnolunate, ulnocapitate, and ulnotriquetral ligaments), midcarpal (triquetrohamate and triquetrocapitate ligaments), and dorsal carpal (dorsal intercarpal and radiotriquetral) ligaments (Figs. 74-5 and 74-6).
The LT ligament is C shaped, spanning the (1) dorsal, (2) proximal, and (3) palmar edges of the joint surfaces. The palmar region is the thickest and strongest. It is the primary stabilizer of the LT joint. Additional supports of the LT joint include the ulnocarpal (ulnolunate, ulnocapitate, and ulnotriquetral ligaments), midcarpal (triquetrohamate and triquetrocapitate ligaments), and dorsal carpal (dorsal intercarpal and radiotriquetral) ligaments (Figs. 74-5 and 74-6).