Fig. 1
(a–c) Pre-operative clinical photographs of the (a) front, (b) side, and (c) back view of the patient showing an equinus deformity of 30°, varus of 20°, as well as claw toe deformities with atrophy of muscles in all compartments of the right leg
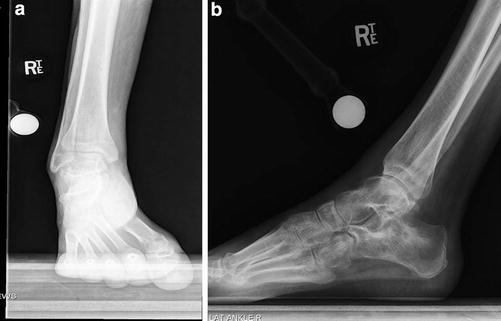
Fig. 2
(a, b) Pre-operative standing ankle: (a) anteroposterior (AP) and (b) lateral radiographs of the right ankle demonstrating the aforementioned equinovarus deformity
3 Preoperative Problem List
1.
Right common peroneal nerve injury with foot drop and sensory deficit
2.
Muscle loss over anterior and lateral compartments of leg
3.
30° equinus contracture right ankle
4.
20° varus contracture right hindfoot
5.
Claw toes
4 Treatment Strategy
1.
Release of tight soft tissue structures contributing to the equinovarus contracture and the claw toes.
2.
Application of TSF for gradual correction of the residual equinovarus contracture after soft tissue releases to achieve complete correction. This is done in two stages: First the foot varus is corrected, and then with modification of the frame, the ankle equinus is corrected.
3.
PTT transfer is planned after TSF removal to achieve active dorsiflexion or at least a tenodesis effect.
5 Basic Principles
1.
Perform a gastrocnemius-soleus recession for the equinus contracture through a minimal posterior incision.
2.
Through a medial ankle/foot approach, release the flexor digitorum longus (FDL) and flexor hallucis longus (FHL) to the knot of Henry. In this particular case, the posterior tibial tendon (PTT) had some motor power on pre-operative clinical exam. Therefore, PTT release was not performed in anticipation for a potential subsequent surgical transfer of the tendon to the dorsum of the foot for management of drop foot. The goal was to attain active dorsiflexion or at least to achieve a tenodesis effect.
3.
Additional percutaneous tenotomies of the flexor tendons were performed with percutaneous K-wire fixation of the distal and proximal interphalangeal joints of the toes and transfixing the K-wires to the TSF.
4.
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Application of TSF with a ring on the distal tibia and a U-ring around the foot. The talar wire was initially attached to the tibial ring (Fig. 3b, yellow arrow) during the correction of the varus deformity. This is because varus correction occurs around the hindfoot axis, necessitating that the tibia and talus be considered as the proximal segment. After full correction of varus, the talar wire was transferred to the foot ring (Fig. 4a, yellow arrow) to correct the equinus contracture, where the talus (with the hind/midfoot) is rotated into dorsiflexion in relation to the ankle mortise of the distal tibia.
Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
