Procedure 73 Scapholunate Ligament Reconstruction Using a Flexor Carpi Radialis Tendon Graft
 See Video 54: Scapholunate Ligament Reconstruction Using the Flexor Carpi Radialis Tendon
See Video 54: Scapholunate Ligament Reconstruction Using the Flexor Carpi Radialis Tendon

Examination/Imaging
Clinical Examination
 Patients complain of radial-sided wrist pain especially with loading activities, weakness of grip, and swelling.
Patients complain of radial-sided wrist pain especially with loading activities, weakness of grip, and swelling.

 Discomfort is reported at extremes of wrist extension and radial deviation.
Discomfort is reported at extremes of wrist extension and radial deviation.
 The scaphoid shift test (Watson test) may be positive in SL dissociation. The examiner places four fingers behind the radius. The thumb is placed on the scaphoid tuberosity, and the other hand is used to move the wrist passively from ulnar to radial deviation. In ulnar deviation, the scaphoid is extended, whereas in radial deviation, the scaphoid is flexed. Pressure on the tuberosity while the wrist is moved from ulnar deviation to radial deviation prevents the scaphoid from flexing. In such circumstances, if the SL ligaments are completely insufficient or torn, the proximal pole subluxates dorsally out of the scaphoid fossa, inducing pain on the dorsoradial aspect of the wrist. When pressure is released, a typical clunk may occur, indicating an abrupt self-reduction of the scaphoid back into its normal position (Fig. 73-1). This test is painful for the patient and should be done selectively, when obvious SL separation is not seen on radiograph.
The scaphoid shift test (Watson test) may be positive in SL dissociation. The examiner places four fingers behind the radius. The thumb is placed on the scaphoid tuberosity, and the other hand is used to move the wrist passively from ulnar to radial deviation. In ulnar deviation, the scaphoid is extended, whereas in radial deviation, the scaphoid is flexed. Pressure on the tuberosity while the wrist is moved from ulnar deviation to radial deviation prevents the scaphoid from flexing. In such circumstances, if the SL ligaments are completely insufficient or torn, the proximal pole subluxates dorsally out of the scaphoid fossa, inducing pain on the dorsoradial aspect of the wrist. When pressure is released, a typical clunk may occur, indicating an abrupt self-reduction of the scaphoid back into its normal position (Fig. 73-1). This test is painful for the patient and should be done selectively, when obvious SL separation is not seen on radiograph.
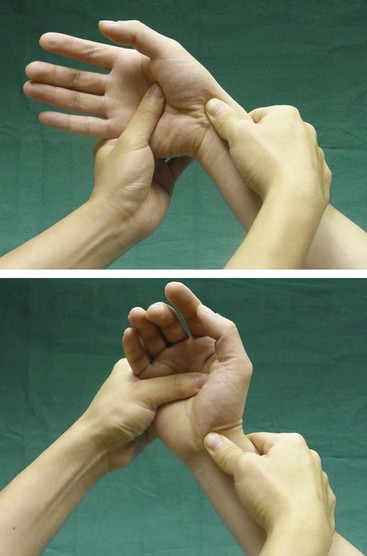
 A positive SL ballottement test may be elicited. The examiner holds the patient’s scaphoid between the thumb (placed over the scaphoid tuberosity on the palmar side) and index finger (placed over the proximal pole of the scaphoid on the dorsum) of one hand, while holding the lunate between the thumb and index of the other hand. The examiner then attempts to move the scaphoid and lunate in opposite directions. If the test induces pain, this test is positive, and the patient may have SL instability (Fig. 73-2).
A positive SL ballottement test may be elicited. The examiner holds the patient’s scaphoid between the thumb (placed over the scaphoid tuberosity on the palmar side) and index finger (placed over the proximal pole of the scaphoid on the dorsum) of one hand, while holding the lunate between the thumb and index of the other hand. The examiner then attempts to move the scaphoid and lunate in opposite directions. If the test induces pain, this test is positive, and the patient may have SL instability (Fig. 73-2).

Imaging
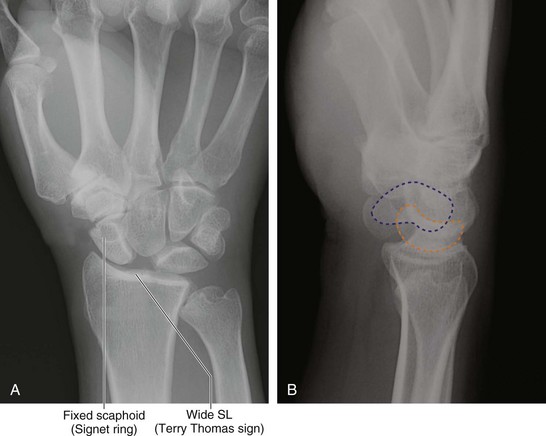
 A gap greater than 3 mm between the scaphoid and lunate on a standard posteroanterior (PA) view indicates SL dissociation. The presence of a flexed scaphoid on a PA view (signet ring sign) (Fig. 73-3A) and an extended lunate on a lateral view is suggestive of SL dissociation with associated carpal malalignment (DISI) (Fig. 73-3B).
A gap greater than 3 mm between the scaphoid and lunate on a standard posteroanterior (PA) view indicates SL dissociation. The presence of a flexed scaphoid on a PA view (signet ring sign) (Fig. 73-3A) and an extended lunate on a lateral view is suggestive of SL dissociation with associated carpal malalignment (DISI) (Fig. 73-3B).
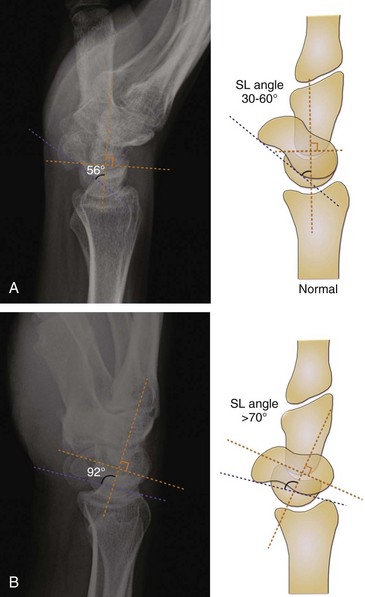
 The normal SL angle ranges from 30 to 60 degrees (Fig. 73-4A). An SL angle greater than 70° indicates DISI (Fig. 73-4B). The SL angle is formed by intersection of the scaphoid axis (a line joining the most palmar point on the distal pole with the most palmar point on the proximal pole of the scaphoid) and lunate axis (a line drawn perpendicular to the line joining the most distal palmar and dorsal points of the lunate).
The normal SL angle ranges from 30 to 60 degrees (Fig. 73-4A). An SL angle greater than 70° indicates DISI (Fig. 73-4B). The SL angle is formed by intersection of the scaphoid axis (a line joining the most palmar point on the distal pole with the most palmar point on the proximal pole of the scaphoid) and lunate axis (a line drawn perpendicular to the line joining the most distal palmar and dorsal points of the lunate).
 The presence of osteoarthritic changes involving the radiocarpal or midcarpal joints is a contraindication for ligament reconstruction. Figure 73-5 shows radiographs of a patient with bilateral SL dissociation. He has osteoarthritic changes involving the radial styloid and radioscaphoid joint on the left side.
The presence of osteoarthritic changes involving the radiocarpal or midcarpal joints is a contraindication for ligament reconstruction. Figure 73-5 shows radiographs of a patient with bilateral SL dissociation. He has osteoarthritic changes involving the radial styloid and radioscaphoid joint on the left side.



Surgical Anatomy
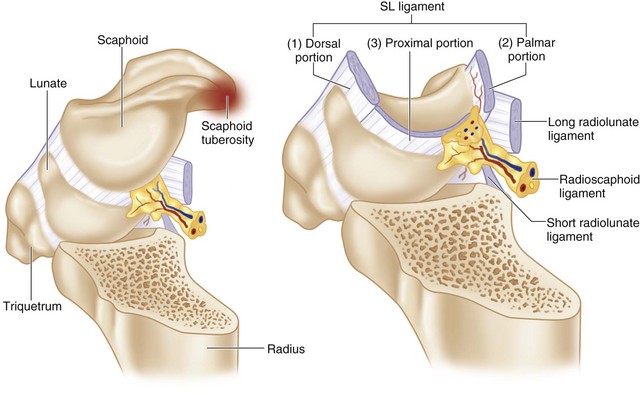
 The SL ligament is a C-shaped structure that connects the dorsal, proximal, and volar surfaces of the scaphoid and lunate. It has three portions: (1) the dorsal portion, which has the highest rupture strength and is responsible for rotational and translational restraint; (2) the proximal membranous portion; and (3) the volar portion (Fig. 73-6).
The SL ligament is a C-shaped structure that connects the dorsal, proximal, and volar surfaces of the scaphoid and lunate. It has three portions: (1) the dorsal portion, which has the highest rupture strength and is responsible for rotational and translational restraint; (2) the proximal membranous portion; and (3) the volar portion (Fig. 73-6).