Procedure 72 Dorsal Capsulodesis for Scapholunate Instability Using Suture Anchors
 See Video 53: Dorsal Capsulodesis for Scapholunate Ligament Injury
See Video 53: Dorsal Capsulodesis for Scapholunate Ligament Injury
Indications
 Static or dynamic dorsal intercalated segmental instability (DISI) deformity is found without a wide scapholunate (SL) gap.
Static or dynamic dorsal intercalated segmental instability (DISI) deformity is found without a wide scapholunate (SL) gap.
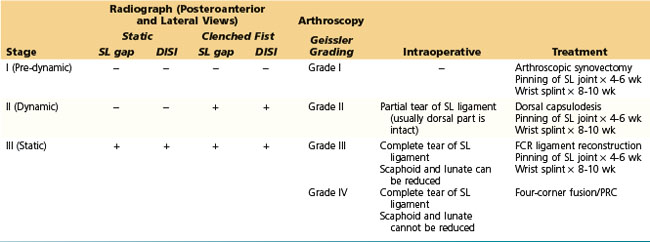
 We determine the treatment for SL instability based on clinical presentation, radiographic appearance, and arthroscopic and intraoperative findings. Our current algorithm for selection of appropriate procedure for SL instability is indicated in Table 72-1.
We determine the treatment for SL instability based on clinical presentation, radiographic appearance, and arthroscopic and intraoperative findings. Our current algorithm for selection of appropriate procedure for SL instability is indicated in Table 72-1.
Examination/Imaging
Clinical Examination
 Patients complain of radial-sided wrist pain especially with loading activities, weakness of grip, and swelling, along with discomfort at extremes of wrist extension and radial deviation.
Patients complain of radial-sided wrist pain especially with loading activities, weakness of grip, and swelling, along with discomfort at extremes of wrist extension and radial deviation.



Imaging
 Stress views, including the clenched-fist view, posteroanterior maximal radial deviation, and posteroanterior maximal ulnar deviation, are useful in the diagnosis of dynamic SL instability.
Stress views, including the clenched-fist view, posteroanterior maximal radial deviation, and posteroanterior maximal ulnar deviation, are useful in the diagnosis of dynamic SL instability.
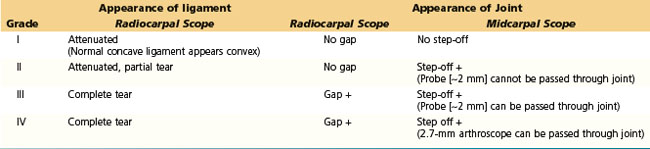
 Arthroscopic examination has become the standard method of evaluation of interosseous ligamentous injuries. The arthroscopic classification of ligament injuries proposed by Geissler (Table 72-2) is useful in determining treatment options.
Arthroscopic examination has become the standard method of evaluation of interosseous ligamentous injuries. The arthroscopic classification of ligament injuries proposed by Geissler (Table 72-2) is useful in determining treatment options.
Surgical Anatomy
 The SL ligament is a C-shaped structure that connects the dorsal, proximal, and volar surfaces of the scaphoid and lunate. Partial SL ligament tears most often involve only the proximal and volar components of the SL interosseous ligament complex. The dorsal ligament is much stronger than its volar counterpart and may resist substantial traumatic torques without yielding.
The SL ligament is a C-shaped structure that connects the dorsal, proximal, and volar surfaces of the scaphoid and lunate. Partial SL ligament tears most often involve only the proximal and volar components of the SL interosseous ligament complex. The dorsal ligament is much stronger than its volar counterpart and may resist substantial traumatic torques without yielding.







