Procedure 7 Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
 See Video 4: Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
See Video 4: Acute Repair of Zone 1 Flexor Digitorum Profundus Avulsion
Indications





Examination/Imaging
Clinical Examination
 With the metacarpophalangeal (MCP) and PIP joints in extension, the patient is unable to actively flex the DIP joint (Fig. 7-1).
With the metacarpophalangeal (MCP) and PIP joints in extension, the patient is unable to actively flex the DIP joint (Fig. 7-1).






Surgical Anatomy
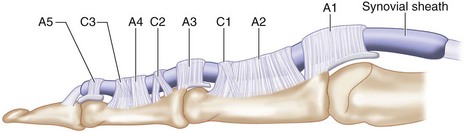
 Flexor zone 1 is distal to flexor digitorum superficialis (FDS) insertion over the middle third of the middle phalanx and contains only the FDP, C3, and A5 pulleys (Fig. 7-3).
Flexor zone 1 is distal to flexor digitorum superficialis (FDS) insertion over the middle third of the middle phalanx and contains only the FDP, C3, and A5 pulleys (Fig. 7-3).
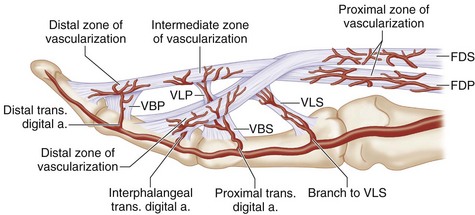
 Blood supply to the distal FDP is from the vinculum longus profundus (VLP), vinculum brevis profundus (VBP), and distal phalanx at its bony insertion (Fig. 7-4).
Blood supply to the distal FDP is from the vinculum longus profundus (VLP), vinculum brevis profundus (VBP), and distal phalanx at its bony insertion (Fig. 7-4).
 Avulsed tendon can retract proximally in three patterns as defined by Leddy and Packer (1977). Additional types 4 and 5 have been described (Fig. 7-5).
Avulsed tendon can retract proximally in three patterns as defined by Leddy and Packer (1977). Additional types 4 and 5 have been described (Fig. 7-5).


Related posts:
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


