Fig. 1
(a) Antero-posterior (AP) radiograph right femur on day of injury. (b) Lateral radiograph right femur on day of injury
3 Preoperative Problem List
1.
Open fracture
2.
Distal femoral fracture with intercondylar extension
3.
Segmental femoral bone loss measuring 12 cm
4 Treatment Strategy
The treatment strategy began with an aggressive debridement to minimize infection risk. Once the soft tissues had stabilized, the surgical options to treat the femoral defect were considered. A long oblique osteotomy and lengthening was decided for this acutely shortened femur. The plan was to perform a lengthening over a nail technique. This patient’s treatment course was as follows: Upon arrival to the hospital, a standard protocol for trauma patients was followed. Once the patient was deemed stable, an emergent debridement, irrigation, and temporary external fixation of all fractures was completed. On hospital day number 12, an acute shortening and femoral internal fixation replaced the external fixator (Fig. 2). This femoral plate remained while the soft tissues healed. At 5 months after injury, the plate was removed, a femoral osteotomy completed and lengthening was initiated. A monorail external fixator distracted the osteotomy site, and a retrograde nail prevented varus angulation. Total time of monorail external fixation was 4 months. Consolidation of the osteotomy continued after monorail removal. The retrograde rod was locked with multiple screws to maintain length achieved by the external fixator monorail.
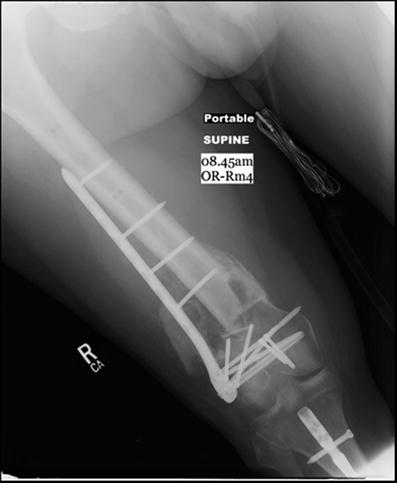
Fig. 2
AP radiograph 5 months after internal fixation
5 Basic Principles
Emergent debridement of the open fractures and external fixation were the initial and primary principles followed to minimize infection risk. Calcium sulphate beads alongside vancomycin and tobramycin were placed in the wounds at the index surgery. Twelve days later, the soft tissues were deemed suitable for internal fixation. The fracture consolidated albeit shortened over the next 5 months. The oblique diaphyseal femoral osteotomy was completed in a stepwise fashion with drill bits and osteotomes to minimize bone necrosis (Fig. 4a, b). Distraction was initiated 10 days after the osteotomy. It was continued at a rate of 1 mm/day (Fig. 5a, b).
6 Images During Treatment
See Figs. 2, 3, 4, and 5.
Fig. 3
 8: Femoral Bone Defect
8: Femoral Bone Defect
 28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
