Procedure 69 Vascularized Bone Grafting for Scaphoid Nonunion
 See Video 51: Pedicled Vascularized Bone Transfer for Scaphoid Nonunion
See Video 51: Pedicled Vascularized Bone Transfer for Scaphoid Nonunion
Indications



Examination/Imaging
Clinical Examination



Imaging
 Wrist radiographs including scaphoid views should be obtained to evaluate the overall fracture pattern, carpal alignment, and degree of radiocarpal and midcarpal arthritis. Chronic scaphoid nonunions display a characteristic pattern of wrist arthritis and carpal instability—scaphoid nonunion advanced collapse (SNAC), as described by Watson and Ballet. The hallmark of AVN on radiographs is increased bone density, fragmentation, and collapse (Fig. 69-1).
Wrist radiographs including scaphoid views should be obtained to evaluate the overall fracture pattern, carpal alignment, and degree of radiocarpal and midcarpal arthritis. Chronic scaphoid nonunions display a characteristic pattern of wrist arthritis and carpal instability—scaphoid nonunion advanced collapse (SNAC), as described by Watson and Ballet. The hallmark of AVN on radiographs is increased bone density, fragmentation, and collapse (Fig. 69-1).

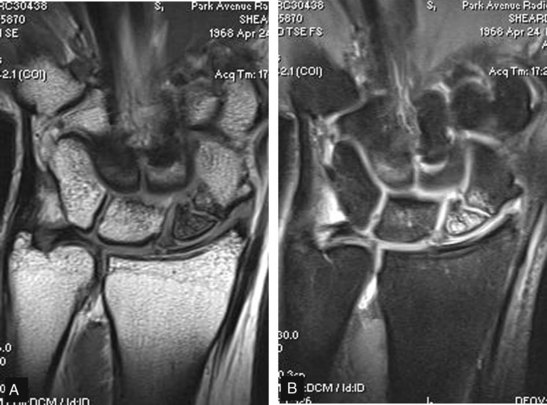
 Magnetic resonance imaging (MRI) is the only noninvasive study able to assess vascularity of the scaphoid and identify AVN (Fig. 69-2). An MRI should be obtained in every patient for whom there is a concern about the viability of the proximal pole. Contrast-enhanced imaging has a sensitivity of 66%, a specificity of 88%, and an accuracy of 83%.
Magnetic resonance imaging (MRI) is the only noninvasive study able to assess vascularity of the scaphoid and identify AVN (Fig. 69-2). An MRI should be obtained in every patient for whom there is a concern about the viability of the proximal pole. Contrast-enhanced imaging has a sensitivity of 66%, a specificity of 88%, and an accuracy of 83%.

Surgical Anatomy
 Eighty percent of the scaphoid surface is covered by articular cartilage, leaving limited space for vascular supply.
Eighty percent of the scaphoid surface is covered by articular cartilage, leaving limited space for vascular supply.
 A dorsal branch of the radial artery provides 70% to 80% of the blood supply.
A dorsal branch of the radial artery provides 70% to 80% of the blood supply.
 A second nutrient artery enters volarly and supplies only the distal pole.
A second nutrient artery enters volarly and supplies only the distal pole.
 There is no nutrient artery to the proximal pole; thus, it is susceptible to AVN when fractured.
There is no nutrient artery to the proximal pole; thus, it is susceptible to AVN when fractured.
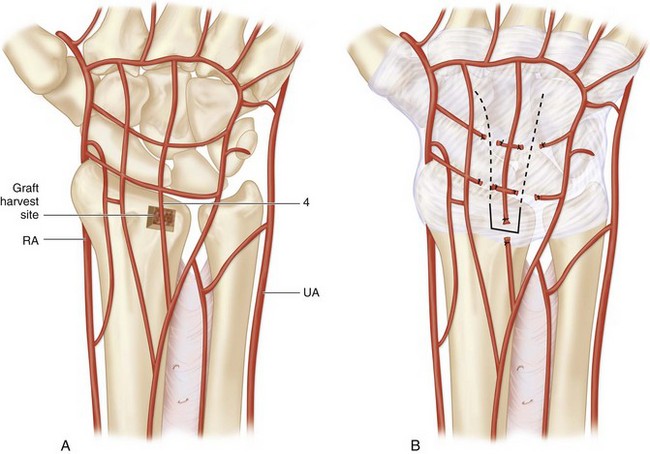
 Dorsal distal-radius vascularized bone grafts have been shown to be based on consistent vascular anatomy (Fig. 69-3A).
Dorsal distal-radius vascularized bone grafts have been shown to be based on consistent vascular anatomy (Fig. 69-3A).
 The pedicled graft described in this chapter is based on the artery of the fourth extensor compartment. The fourth extensor compartment artery is less than 1 mm in diameter and between 1 and 2 cm in length (see Fig. 69-3A and B).
The pedicled graft described in this chapter is based on the artery of the fourth extensor compartment. The fourth extensor compartment artery is less than 1 mm in diameter and between 1 and 2 cm in length (see Fig. 69-3A and B).