Procedure 68 Percutaneous Screw Fixation of Scaphoid Fractures
 See Video 50: Screw Fixation of Scaphoid Fracture
See Video 50: Screw Fixation of Scaphoid Fracture



Examination/Imaging
Clinical Examination
 Fractures of scaphoid are frequently missed in the emergency room or dismissed by the patient as a wrist sprain. Thus, the physician must have a high suspicion in young and middle-aged patients who present with wrist pain after a fall on an outstretched hand.
Fractures of scaphoid are frequently missed in the emergency room or dismissed by the patient as a wrist sprain. Thus, the physician must have a high suspicion in young and middle-aged patients who present with wrist pain after a fall on an outstretched hand.
 General dorsoradial edema and focal snuffbox tenderness are highly suggestive of an acute scaphoid fracture (Fig. 68-1).
General dorsoradial edema and focal snuffbox tenderness are highly suggestive of an acute scaphoid fracture (Fig. 68-1).
 The distal pole of scaphoid may be tender to palpation (Fig. 68-2).
The distal pole of scaphoid may be tender to palpation (Fig. 68-2).



Imaging
 The initial posteroanterior (PA) and lateral radiographs may fail to demonstrate a scaphoid fracture (Fig. 68-3). The incidence of false-negative radiographs for acute fractures has been shown to be up to 25%.
The initial posteroanterior (PA) and lateral radiographs may fail to demonstrate a scaphoid fracture (Fig. 68-3). The incidence of false-negative radiographs for acute fractures has been shown to be up to 25%.
 Additional helpful radiographic views include (1) clenched-fist PA, which can exaggerate a fracture deformity and help make a diagnosis; (2) ulnar-deviated PA that positions the scaphoid in extension showing the waist more clearly (Fig. 68-4); and (3) pronated oblique view.
Additional helpful radiographic views include (1) clenched-fist PA, which can exaggerate a fracture deformity and help make a diagnosis; (2) ulnar-deviated PA that positions the scaphoid in extension showing the waist more clearly (Fig. 68-4); and (3) pronated oblique view.
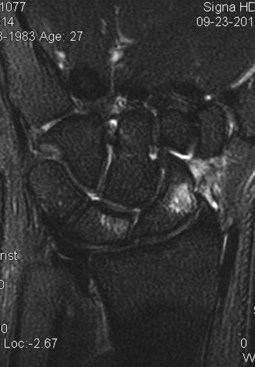
 Magnetic resonance imaging (MRI) is highly sensitive for making the diagnosis—cortical disruption with bone marrow edema is diagnostic. For chronic injuries, MRI is valuable in assessing proximal pole vascularity (Fig. 68-5).
Magnetic resonance imaging (MRI) is highly sensitive for making the diagnosis—cortical disruption with bone marrow edema is diagnostic. For chronic injuries, MRI is valuable in assessing proximal pole vascularity (Fig. 68-5).



Surgical Anatomy
 The scaphoid is the largest bone in the proximal carpal row, and its axis lies about 45 degrees to the longitudinal axis of the wrist.
The scaphoid is the largest bone in the proximal carpal row, and its axis lies about 45 degrees to the longitudinal axis of the wrist.


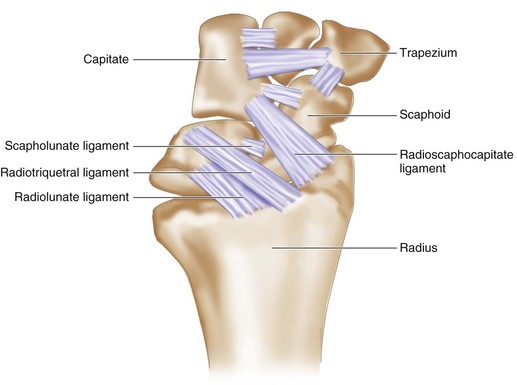
 Multiple intrinsic and extrinsic ligaments attach to the scaphoid (Fig. 68-6). The most important is the radioscaphocapitate, which provides an axis on which the scaphoid flexes.
Multiple intrinsic and extrinsic ligaments attach to the scaphoid (Fig. 68-6). The most important is the radioscaphocapitate, which provides an axis on which the scaphoid flexes.

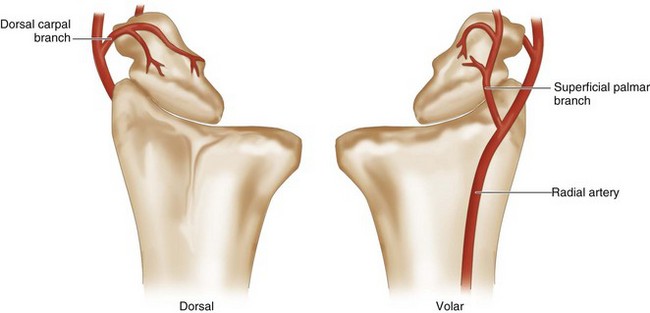
 A dorsal branch of the radial artery provides 70% to 80% of the blood supply (Fig. 68-7).
A dorsal branch of the radial artery provides 70% to 80% of the blood supply (Fig. 68-7).
 A second nutrient artery enters volarly and supplies only the distal pole.
A second nutrient artery enters volarly and supplies only the distal pole.

Positioning
 The patient is positioned supine on the operating room table with the arm abducted on a radiolucent hand table.
The patient is positioned supine on the operating room table with the arm abducted on a radiolucent hand table.

Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


