Procedure 64 Diagnostic Wrist Arthroscopy
 See Video 48: Diagnostic Wrist Arthroscopy
See Video 48: Diagnostic Wrist Arthroscopy
Indications
 Patients who have objective mechanical pathology of the wrist
Patients who have objective mechanical pathology of the wrist


Examination/Imaging
Clinical Examination
 Arthroscopy has revolutionized the practice of hand surgery by providing the capability to examine and treat intra-articular abnormalities. Development of wrist arthroscopy is a natural transition from the successful application of arthroscopy of the larger joints. Wrist arthroscopy has seen considerable growth since Whipple reported the original description of the technique he developed for reviewing the intra-articular anatomy of the joints.
Arthroscopy has revolutionized the practice of hand surgery by providing the capability to examine and treat intra-articular abnormalities. Development of wrist arthroscopy is a natural transition from the successful application of arthroscopy of the larger joints. Wrist arthroscopy has seen considerable growth since Whipple reported the original description of the technique he developed for reviewing the intra-articular anatomy of the joints.

 Patients with injury to the TFCC complain of pain at the head of the ulna or the prestyloid recess.
Patients with injury to the TFCC complain of pain at the head of the ulna or the prestyloid recess.
 Patients with fractures of the scaphoid are tender in the snuffbox.
Patients with fractures of the scaphoid are tender in the snuffbox.




Surgical Anatomy
 The wrist is the labyrinth of eight carpal bones. Multiple articular surfaces with intrinsic and extrinsic ligaments and the TFCC form a perplexing joint that continuously challenges physicians with an array of diagnoses. Wrist arthroscopy allows direct visualization of the cartilage surfaces, carpal bones, and ligaments using bright light and magnification.
The wrist is the labyrinth of eight carpal bones. Multiple articular surfaces with intrinsic and extrinsic ligaments and the TFCC form a perplexing joint that continuously challenges physicians with an array of diagnoses. Wrist arthroscopy allows direct visualization of the cartilage surfaces, carpal bones, and ligaments using bright light and magnification.

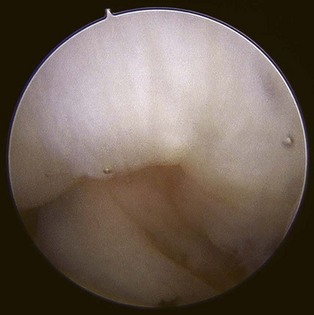
 Geissler defined an arthroscopic classification for interosseous ligament injury. A spectrum of injury is seen throughout this ligament. The ligament stretches and then tears, usually in a volar to dorsal direction. This arthroscopic classification is based on evaluation of the interosseous ligament from both the radiocarpal and midcarpal spaces. (Fig. 64-1 shows arthroscopic view of a normal scapholunate ligament.)
Geissler defined an arthroscopic classification for interosseous ligament injury. A spectrum of injury is seen throughout this ligament. The ligament stretches and then tears, usually in a volar to dorsal direction. This arthroscopic classification is based on evaluation of the interosseous ligament from both the radiocarpal and midcarpal spaces. (Fig. 64-1 shows arthroscopic view of a normal scapholunate ligament.)



Exposures
 Wrist arthroscopy portals are made according to the space to which they correspond with respect to the extensor compartments (Fig. 64-6).
Wrist arthroscopy portals are made according to the space to which they correspond with respect to the extensor compartments (Fig. 64-6).
 The traditional portal is the 3-4 portal. This portal is made between the third and fourth dorsal compartments of the wrist. The 3-4 portal is located by palpating Lister tubercle by advancing the finger about 1 cm distal until the soft spot is noted over the dorsal lip of the radius. The 3-4 portal is in line with the radial border of the long finger. (Fig. 64-7
The traditional portal is the 3-4 portal. This portal is made between the third and fourth dorsal compartments of the wrist. The 3-4 portal is located by palpating Lister tubercle by advancing the finger about 1 cm distal until the soft spot is noted over the dorsal lip of the radius. The 3-4 portal is in line with the radial border of the long finger. (Fig. 64-7
Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


