Procedure 63 Trapeziometacarpal Fusion
 See Video 47: Fusion of Thumb Carpometacarpal Joint
See Video 47: Fusion of Thumb Carpometacarpal Joint
Indications
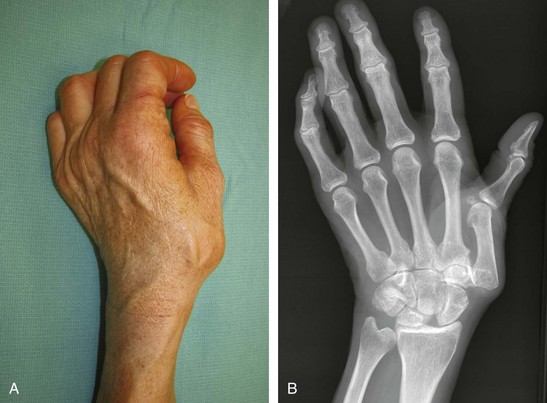
 Posttraumatic degenerative osteoarthritis of the trapeziometacarpal (TMC) joint in manual workers who require great stability of the carpometacarpal (CMC) joint, which may not be achieved with trapezium excision and ligament reconstruction
Posttraumatic degenerative osteoarthritis of the trapeziometacarpal (TMC) joint in manual workers who require great stability of the carpometacarpal (CMC) joint, which may not be achieved with trapezium excision and ligament reconstruction