Procedure 6 Surgical Treatment of de Quervain Tendovaginitis
 See Video 3: Release of First Dorsal Compartment for de Quervain Tendovaginitis
See Video 3: Release of First Dorsal Compartment for de Quervain Tendovaginitis

Examination/Imaging
Clinical Examination
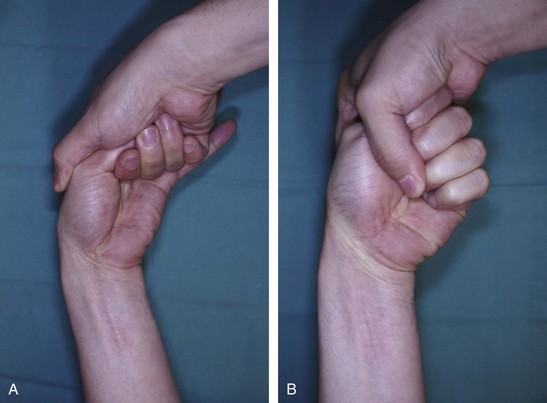
 The patient has tenderness over the radial styloid and may have triggering of the thumb extensor tendons. The following two tests can be done to confirm the presence of de Quervain disease.
The patient has tenderness over the radial styloid and may have triggering of the thumb extensor tendons. The following two tests can be done to confirm the presence of de Quervain disease.



Surgical Anatomy
 Six extensor compartments have been described over the dorsum of the wrist (Fig. 6-3A).
Six extensor compartments have been described over the dorsum of the wrist (Fig. 6-3A).
 The first dorsal compartment is involved in de Quervain tendovaginitis. It contains two tendons, the APL and the EBP (Fig. 6-3B and C). The APL tendon has multiple slips. The APL tendon is more radial and volar, whereas the EPB tendon is ulnar and dorsal. In up to 40% of subjects, there may be a separate subsheath for each of the two tendons.
The first dorsal compartment is involved in de Quervain tendovaginitis. It contains two tendons, the APL and the EBP (Fig. 6-3B and C). The APL tendon has multiple slips. The APL tendon is more radial and volar, whereas the EPB tendon is ulnar and dorsal. In up to 40% of subjects, there may be a separate subsheath for each of the two tendons.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


