Fig. 1
(a) Antero-posterior (AP) radiograph of the right femur on day of injury. (b) Lateral radiograph of the right femur on day of injury

Fig. 2
Radiograph after debridement with oscillating saw and external fixation application
3 Preoperative Problem List
1.
Grossly contaminated right open femur fracture.
2.
Distal femoral fracture with intercondylar extension.
3.
Segmental femoral bone loss measuring 10 cm.
4.
Residual leg length inequality of 3 cm.
4 Treatment Strategy
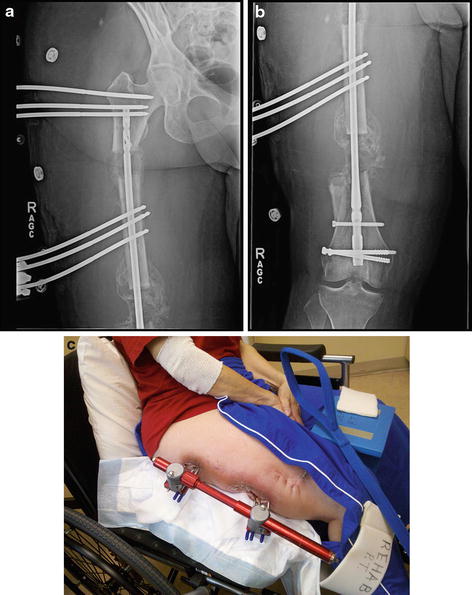
The treatment strategy began with an aggressive debridement to minimize infection risk. Once the soft tissues had stabilized, the surgical options to treat the femoral defect were considered. A significant segment of femur was missing distally, so a transverse subtrochanteric osteotomy was planned (Fig. 3a). The proximal femoral segment would then be transported by external fixation over a femoral nail. On hospital day number 6, an osteotomy was performed, and a monotube external fixator and a retrograde femoral nail were placed (Fig. 3a–c). The surgical plan was to transport the proximal femur into the distal defect (Fig. 4a, b). After 2 months of transport, the distal defect spontaneously healed, and no further transport was required (Fig. 5a–c). The femoral cortices were reconstituted, continuous and tolerant of full weight-bearing. The patient noticed several months later that her leg was short 3 cm. She requested a lengthening procedure, which required 4 months to complete.
Get Clinical Tree app for offline access
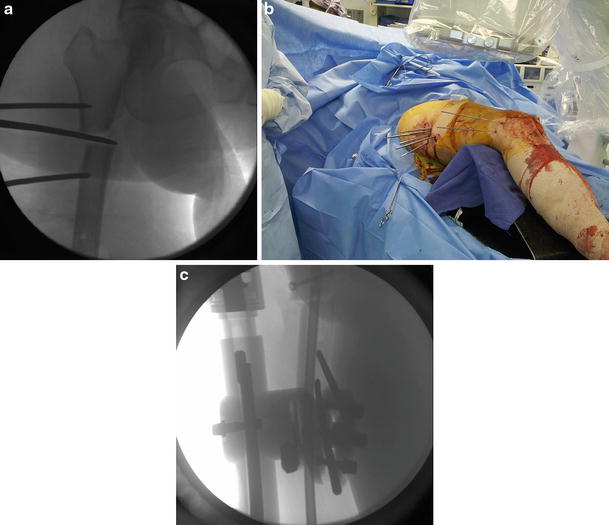
Fig. 3
(a) Intra-operative fluoroscopy demonstrating completion of drill bit osteotomy technique with an osteotome. (b) Intra-operative photograph demonstrating use of five drill bits to perform osteotomy. Each drill bit stays in place as a point of reference for further drilling. Half pins are proximal and distal to the osteotomy. (c) Intra-operative fluoroscopy demonstrating half pins in transport segment behind the rod
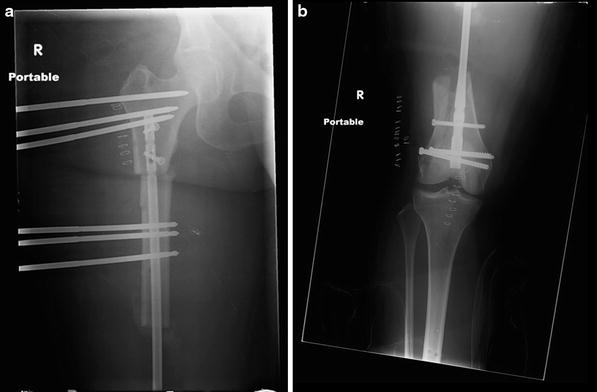
Fig. 4
(a) Radiograph of proximal femur immediately after osteotomy for femoral transport. (b) Radiograph of knee immediately after osteotomy for femoral transport
Fig. 5
(a
 8: Femoral Bone Defect
8: Femoral Bone Defect
 28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
