Procedure 57 Open Reduction of Metacarpophalangeal Joint Dislocation

Examination/Imaging
Clinical Examination
 The MCP joint region will be swollen and tender.
The MCP joint region will be swollen and tender.

 Simple subluxation should be distinguished from a complete dislocation.
Simple subluxation should be distinguished from a complete dislocation.
 In simple subluxation, the proximal phalanx is locked in a hyperextended position (Fig. 57-1).
In simple subluxation, the proximal phalanx is locked in a hyperextended position (Fig. 57-1).
 In a complete dislocation, the proximal phalanx may be less hyperextended and may even be in a bayoneted position (Fig. 57-2).
In a complete dislocation, the proximal phalanx may be less hyperextended and may even be in a bayoneted position (Fig. 57-2).






Surgical Anatomy
 The MCP volar plate has a weaker proximal insertion and tends to avulse from the metacarpal, remaining attached to the base of the proximal phalanx.
The MCP volar plate has a weaker proximal insertion and tends to avulse from the metacarpal, remaining attached to the base of the proximal phalanx.
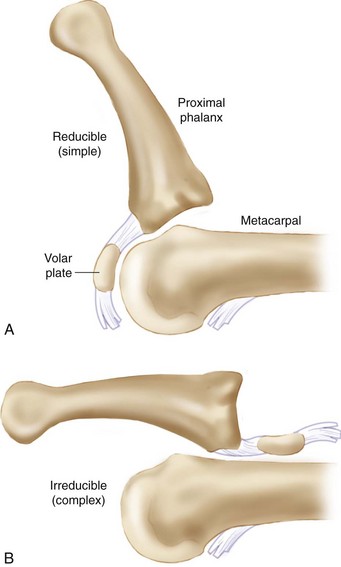
 In a simple subluxation, the proximal phalanx is hyperextended. In this case, the volar plate remains draped over the articular surface of the metacarpal head and does not lie on the dorsal cortex of the metacarpal head (Fig. 57-4A).
In a simple subluxation, the proximal phalanx is hyperextended. In this case, the volar plate remains draped over the articular surface of the metacarpal head and does not lie on the dorsal cortex of the metacarpal head (Fig. 57-4A).
 In a complete or complex dislocation, the proximal phalanx is less hyperextended and may be in a bayonet position. In this case, the volar plate is no longer draped over the metacarpal articular surface but rather lies completely dorsal to the metacarpal head (Fig. 57-4B).
In a complete or complex dislocation, the proximal phalanx is less hyperextended and may be in a bayonet position. In this case, the volar plate is no longer draped over the metacarpal articular surface but rather lies completely dorsal to the metacarpal head (Fig. 57-4B).
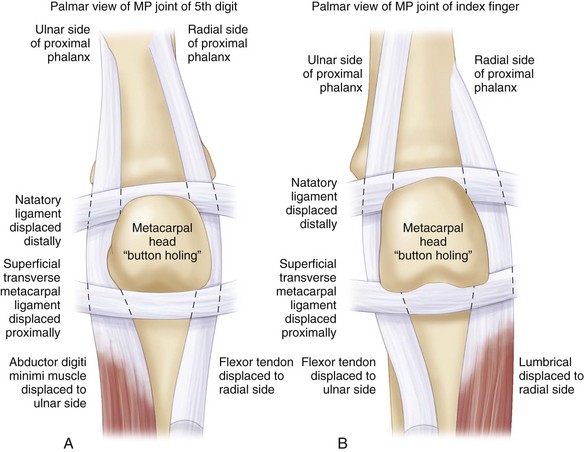
 The dislocation is made complex (irreducible) not only by the volar plate but also by the flexor tendons and lumbrical, which form a noose around the metacarpal neck (Fig. 57-5).
The dislocation is made complex (irreducible) not only by the volar plate but also by the flexor tendons and lumbrical, which form a noose around the metacarpal neck (Fig. 57-5).