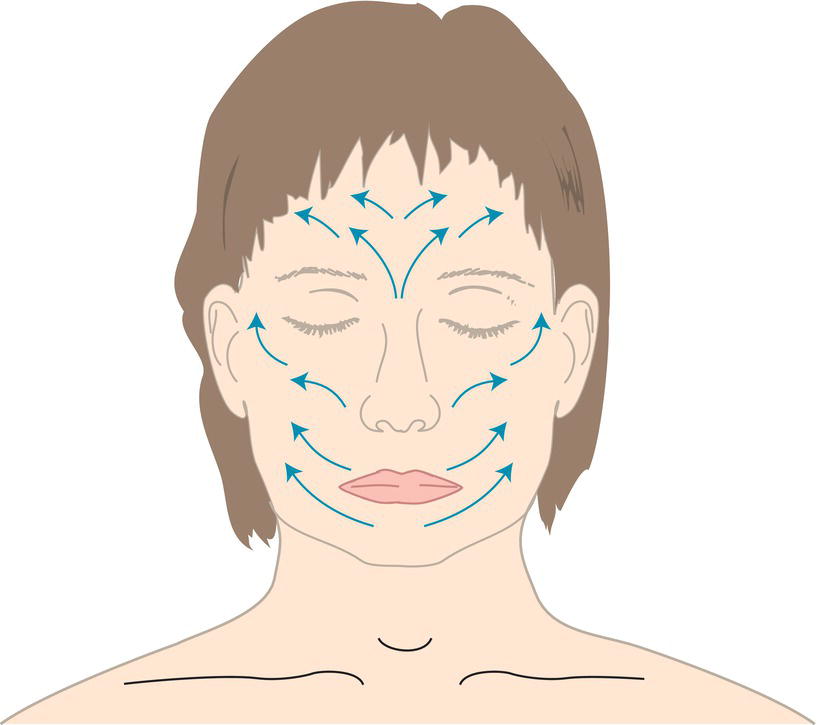
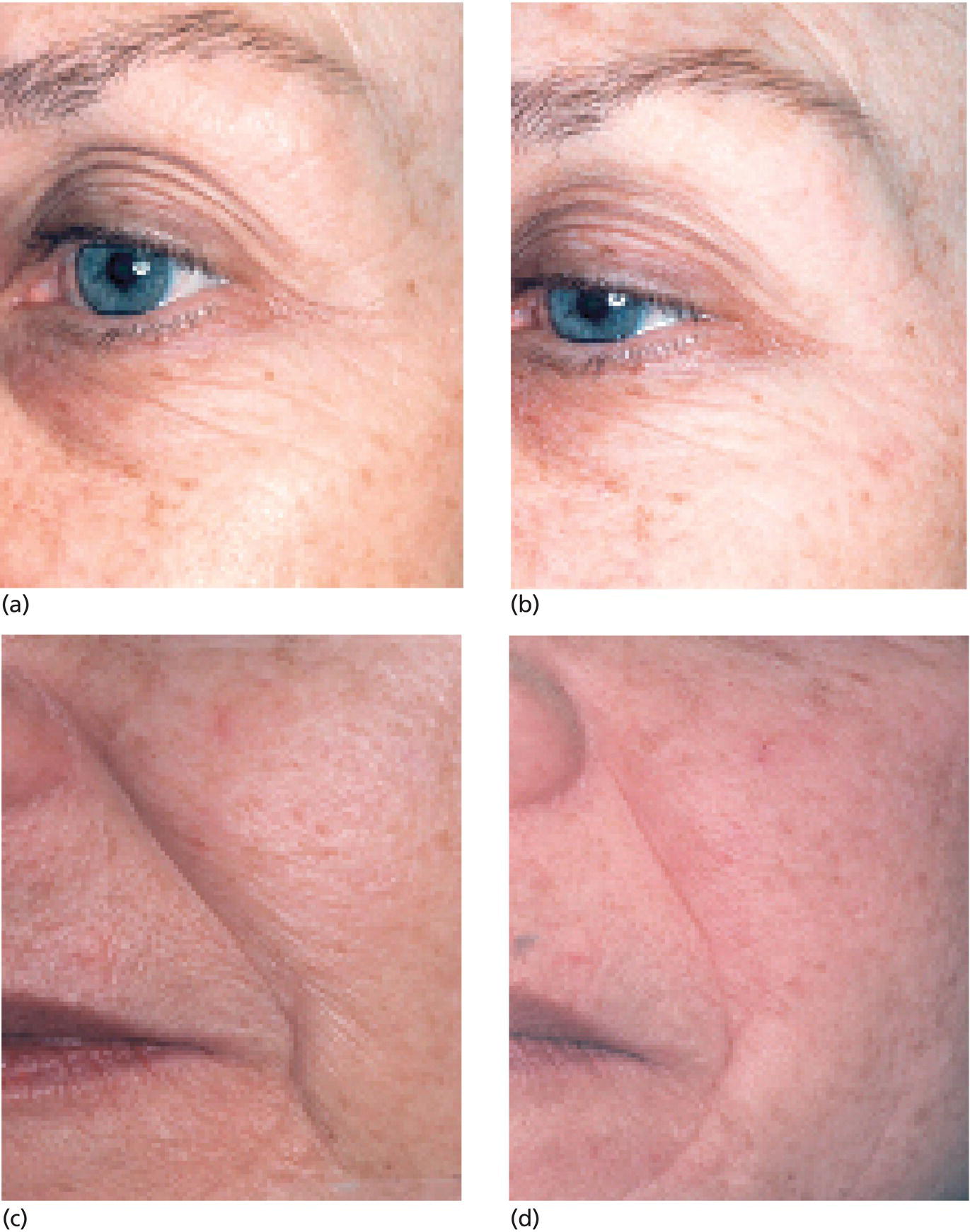
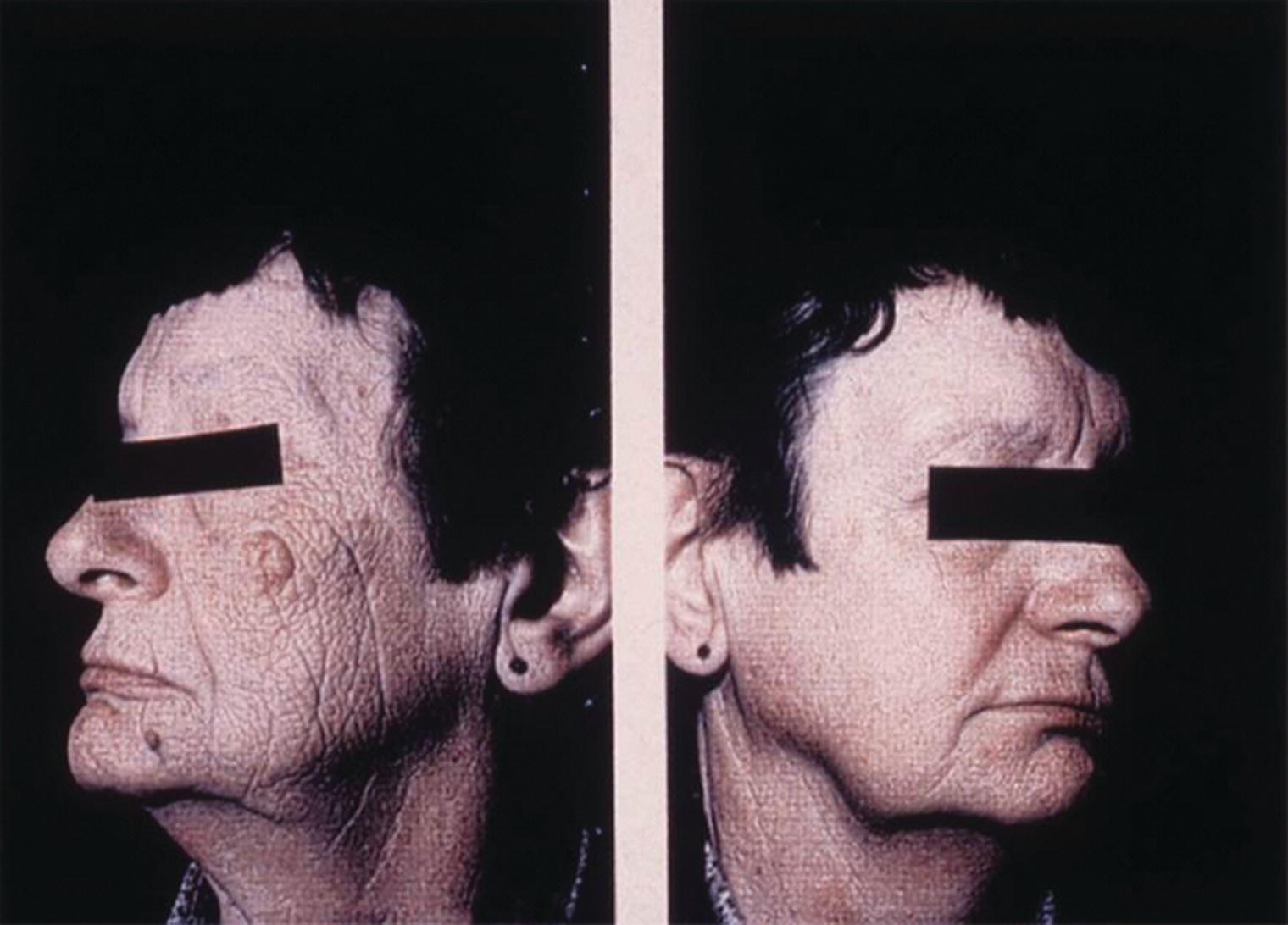
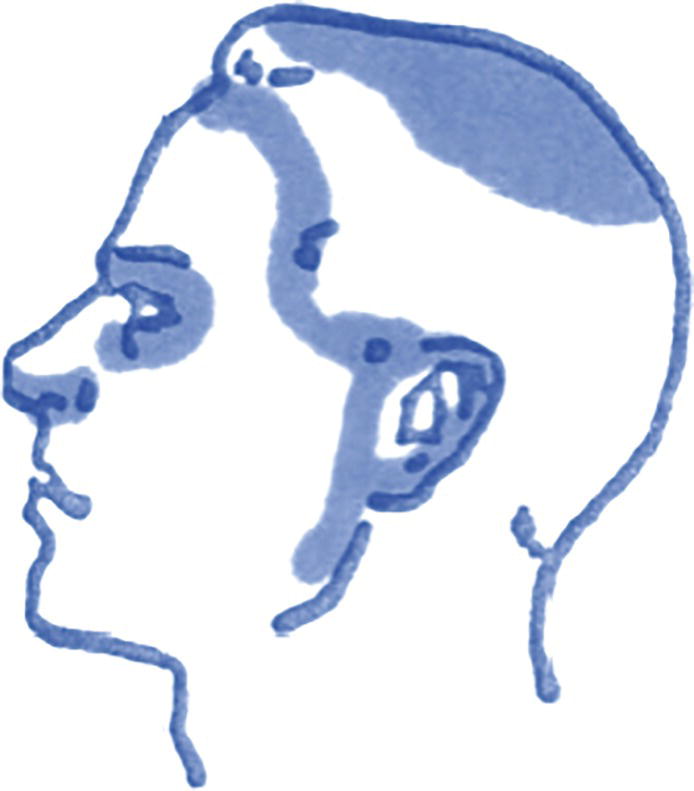
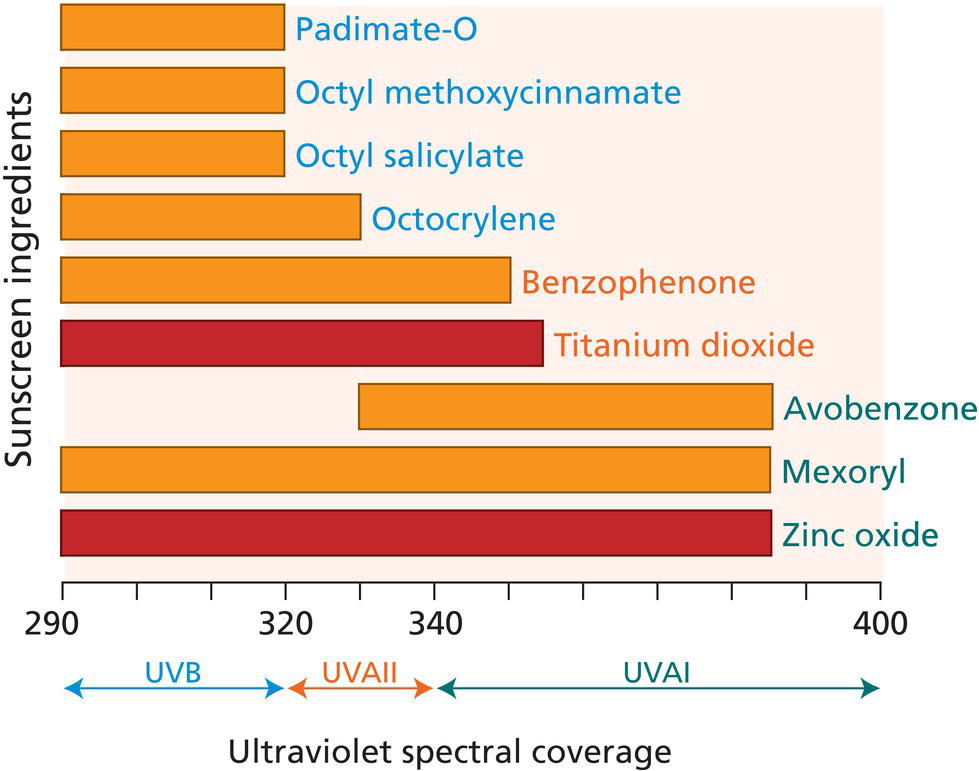
Karen E. Burke The Mount Sinai Medical Center, New York, NY, USA In her book, Survival of the Prettiest, Etcoff [1] synthesizes literature and research from anthropology, biology, psychology, and archeology to show that indeed appreciation of one’s own and others’ beauty is hardwired in human brains. Etcoff concludes, “Flawless skin is the most universally desired feature of beauty.” This chapter presents a basic skin regimen to protect from photodamage and to reverse the appearance of aging. The four necessary steps are cleansing, exfoliation, protection, and treatment. Helpful techniques and scientific research proving efficacy of specific ingredients are presented. Proper cleansing is an essential component of skincare. The face accumulates endogenous and exogenous soils. Sebaceous gland size and density are greatest on the face, upper back, and chest. The natural oils, sweat, and sebum secretions create a hydrolipid film on the skin surface that, in addition to applied cosmetics, traps and accumulates environmental pollutants such as dust, airborne irritants, and compounds from cigarette smoke. Care must be taken to accomplish thorough cleansing, without irritation or drying. Therefore, a gentle, effective cleanser is of utmost importance. Surfactants are the ingredients that bind to dirt and oil for removal. These surfactants are classified by their charge on the surface‐active moiety as anionic (negatively charged, for good foaming and lathering), cationic (positively charged), amphoteric (both positive and negative, considered to “condition” skin while helping to foam), and nonionic (which are used in baby products to suppress foam) [2]. Components of surfactants can bind to the stratum corneum proteins, decreasing the skin’s ability to bind and hold water. With continued, frequent use, surfactants can damage the skin barrier. New synthetic surfactants improve cleansing with less irritation. Other components of cleansers include polypeptides and synthetic polymers to make the product smooth and to soften skin, polymers to moisturize, preservatives, opacifying agents, and fragrance. With frequent washing, these ingredients can cause sensitivities or contact allergy in certain individuals. Because cleansers are rinsed off, their contact time with the skin is reduced causing less contact allergy. Newer cleansers are less alkaline than older formulations, so they are less drying. The inclusion of medications as components of cleansers can be effective in actually treating the skin. To assure efficacy, the cleanser must remain on the skin’s surface for several minutes (at least 2–3 minutes) before rinsing. Salicylic acid, a β‐hydroxy acid, is keratolytic, ungluing dead surface corneocytes thus removing keratin debris from the orifices of pores (1) to reduce pore dilation, thereby decreasing the unattractive appearance of large pores, (2) to prevent and treat open comedones (“blackheads”), and (3) to prevent the keratin plug from initiating the cycle that leads to the comedones and pustules of acne. Keratolysis also smooths small surface wrinkles. Benzoyl peroxide cleansers effectively treat and prevent acne. Use of benzoyl peroxides in cleansers are less irritating and drying than application of benzoyl peroxide creams or gels. Also, since the benzoyl peroxide creams and gels remain on the face, clothes, towels, bedding, and even hair can be bleached with contact, especially if applied at night. Since the benzoyl peroxide in cleansers is removed with rinsing, this bleaching is prevented. Finally, selenium sulfide cleansers (formulated by prescription as 2.5% or as available over‐the‐counter as 2.0% in Selsun Blue shampoo) effectively treat tinea versicolor if used daily for three to four weeks. Individuals who acquire tinea versicolor repeatedly when in hot climates should use selenium sulfide cleansers at least twice per week to prevent recurrence, optimally applying for at least ten minutes before rinsing off – preferably with a body brush to enhance surface exfoliation. In recent years, antibacterial agents (e.g. triclosan and triclocarban) have been added to hand cleansers. Surprisingly, these agents are rarely skin irritants. However, some physicians voice concern, fearing development of bacterial resistance to these antibiotics with frequent use. Originally, triclosan was thought to kill bacteria by a “broad‐based” mechanism, similar to alcohol and peroxide. However, recent research demonstrated that triclosan acts at a specific gene site in Escherichia coli to inhibit replication, so resistant strains could evolve [3]. Thorough washing with gentle cleansers removes dirt and has been shown to be as effective as using these antibacterial compounds. Cleansing the face should be accomplished with lukewarm water and the fingertips. The face and neck should be washed with upward, outward motions. On the face, one should always rub perpendicular to the direction of those wrinkles that could develop later. On the forehead, cheeks, chin and neck, rub up and out; above the upper lip and under the eyes, the strokes should be first horizontal, then upward at the edges, as illustrated in Figure 56.1. Sunscreen, moisturizer, or other treatments should be applied immediately after gently towel‐drying to seal in the water remaining on the skin’s surface. Figure 56.1 To treat wrinkles while washing, gently rub upward horizontally across the upper lip and “up and out” on the rest of the face – perpendicular to the direction of wrinkles. During the COVID‐19 pandemic, the importance of hand washing has come to the forefront, especially after being outside one’s own home, before, during, and after preparing food (especially raw food) and before eating, after putting on shoes, and after touching computers, telephones, tables, countertops, cash bills and coins, packages, magazines, newspapers, doorknobs – all objects touched by others. In public places, use a hand towel to turn on and off spickets. Wash all surfaces of both hands (especially fingertips and between fingers) with a generous amount of soap for at least 20–30 seconds (sing “Happy Birthday” silently once or twice!), then rinse. Also using a hand brush (even a toothbrush “dedicated” to hands) to clean nails thoroughly is advised. If no soap and water are available after touching publicly used objects (door handles, elevator buttons, and seatbelts), alcohol wipes with at least 60–70% isopropyl alcohol does kill cold, flu, and coronavirus by dissolving cellular lipids and denaturing proteins. Higher concentrations of ≥90% isopropyl alcohol are not as effective since the alcohol evaporates too rapidly to penetrate the cell wall to kill the infectious organism; if not evaporated, this high percentage breaks down only the outer cell wall without entering the cell to deliver lethal damage. According to some products’ labels, benzalkonium chloride does “kill 99% of illness‐causing germs,” but this has not yet been tested on coronavirus and may not be effective. Whiskey and vodka do not have sufficient alcohol content to be lethal to bacteria, fungi, or viruses! With this frequent handwashing, hands become dry and eczema flares. Always moisturize hands immediately after towel drying to seal water into surface pores. Use sunscreen formulations during the day and moisturizers after dusk. Carry a small, refillable jar with your preferred products to use frequently. Exfoliation is the rejuvenation treatment providing the most immediate improvement in appearance. Exfoliation removes the outer layers of stratum corneum, and thus treats the hyperkeratosis of dry skin. Exfoliative rubbing perpendicular to the direction of wrinkles (with upward, outward strokes) minimizes small wrinkles because the surface is smoothed (Figure 56.1). Exfoliation can be chemical or mechanical. Chemical exfoliants such as hydroxyacids (HA) and retinoic acid remove dead surface cells by keratolysis. Mechanical exfoliants include cleansing grains, waxy creams that adhere to the surface cells, as well as slightly abrasive terry washcloths, non‐woven polyester polishing pads, brushes, loofas, or mechanical brushes – all of which physically “sand” the skin surface by rubbing. Grainy exfoliants with aluminum oxide crystals can be effective, but the user must be careful not to get the grains into the eyes. Exfoliants to be avoided are those with apricot or almond kernels, walnut shells, and pumice – all of which have irregularly shaped particles with sharp edges which can be too rough for delicate skin and dangerous if they get into the eyes. The immediate improvement in small wrinkles by gentle exfoliation can be appreciated in Figure 56.2. Figure 56.2 Tiny wrinkles and crepey skin can be treated immediately at home by exfoliation. Improvement is seen in this 60‐year‐old woman’s face after she simply washed with a nonwoven polyester polishing pad and used a waxy exfoliant that mechanically “sticks” and removes surface cells. (a) and (c) Pre‐exfoliation; (b) and (d), post‐exfoliation. Masks are among the oldest face mechanical exfoliants. Masks can be “wash‐off” or “peel‐off.” Some “wash‐off” masks are made of clay, which harden and are removed with water rinsing. “Peel‐off” masks contain synthetic polymers that are quite safe and effective. Some masks may irritate the skin; it is advisable to test on the inner wrist before treating the face. The single most effective therapy for aging skin is sun protection [4]. Avoid sun exposure between 10 AM and 4 PM, and beware of “hidden sun”: UVA is not filtered by window glass and neither UVA nor UVB are filtered by clouds. People get their worst burns on cloudy days, especially when skiing at high altitudes or when on the beach or in the water when reflected rays can almost double exposure. If one’s indoor workspace is in direct sun, that person can become sun‐burned through the window and suffer severe photoaging, as seen in Figure 56.3. The unfiltered UVA can also cause a photoallergic dermatitis, which is quite specific to the susceptible individual who has no allergy unless exposed to UVA (from the sun or tanning booths) after topical application of a product containing a particular photosensitizing ingredient such as fragrances (oil of bergamot or lime) or oral intake of a photosensitizing medication (such as an antibiotic (especially those in the tetracycline family), antidepressant, tranquilizer, or diuretic). The possibility of photoallergy makes tanning beds not only harmful, but also dangerous! Some burns after indoor tanning have even been lethal, since the photoallergy is not known until after intense UVA exposure. Even when inside if exposed to UVA through a window, sunscreen should be applied often and generously every 90 minutes. Frequently missed areas with sunscreen application are just in front of and on the ears, around the eyes and on the eyelids, above the lips, on the scalp under thinning hair, on fingertips, and on the neck and upper chest and back as illustrated in Figure 56.4. Figure 56.3 This secretary sat at the same desk for more than 30 years. Her left face which was exposed to UVA through the window shows severe photodamage, especially when compared with the less‐exposed right side. (Source: Photograph courtesy of Michelle Verschoore, L’Oréal Advanced Research Laboratories, Clichy and Aulnay‐Sous‐Bois, France, and Pierre Moulin, Lyon France.) Figure 56.4 Areas where sunscreen is often not adequately applied, as well as on the fingertips, neck, upper chest, and back. Sunscreens are classified as organic filters (which absorb photons of UV light) or inorganic filters (which reflect or scatter UV radiation) [5]. As shown in Figure 56.5, some organic sunscreen agents block only UVB (p‐aminobenzoic acid [PABA] and its esters padamate A and O, the cinnamates, and salicylates); others absorb primarily UVB and some low wavelength UVA (octocrylene, benzophenones, and anthranalides). Ecamsule, sold under the trade name Mexoryl™ XL or SL (Anthelios, La Roche‐Posay, L’Oréal), blocks most UVA as well as UVB. The UVA absorbing sunscreen avobenzone (Parsol 1789) can degrade with exposure to UV [6], but stabilizing compounds (benzylidene camphor and diphenyl cyanoecrylate derivatives, both UVB filters) can be effectively added (Helioplex™, Neutrogena) [7]. The inorganic filters with microfine titanium dioxide and zinc oxide are total UVB blocks, blocking low wavelength UVA and almost all UVA, respectively. Thus, zinc oxide provides better protection than titanium dioxide [8]. The new technology with microfine particles makes them nonopaque and cosmetically appealing. The concentration and the size of the microparticles determine SPF efficacy [5] 1. Figure 56.5 Ultraviolet spectral coverage of sunscreen ingredients. A recent publication in JAMA by the Federal Drug Administration (FDA), physicians created controversy about the use of several sunscreen ingredients (oxybenzone (also named benzophenone‐3), octocrytane, and avobenzone) because nanogram (ng = 10−9 gm) amounts were measurable in plasma after application in human volunteers of maximal doses (more than four times the dose usually applied). These authors raised alarm because the 0.5 ng/mL – the theoretical “highest plasma level below which the carcinogenic risk of any unknown compound would be less than 1 in 100,000 after a single dose was exceeded” [9]. Merely having higher plasma levels than this miniscule amount has never shown any clinical risk [10]. Nevertheless, this led to the FDA’s establishing in 2019 a new designation for sunscreen ingredients “Generally Recognized as Safe and Effective (acronym GRASE) [11] for which only micronized zinc oxide and titanium dioxide qualify. However, subcutis levels even of these inorganic sunscreen components have been measured after application [12]. Another concern is the misguided notion that oxybenzone has caused bleaching of coral reefs in Hawaii and the US Virgin Islands, based on in vitro experiments that demonstrated bleaching of coral at concentrations of 35–55 parts per million (ppm) [13]. This conclusion is not valid. Maximal concentrations measured in the coastal seas of Hawaii and the Virgin Islands are only 0.019 and 1.4 ppm, respectively [14]: these low levels are quite unlikely to cause damage. It is more likely that the coral bleaching is the result of increased water temperatures from global warming which promotes viral infection of the algae Zooxantheliae that lives symbiotically on coral and is necessary for coral photosynthesis [15]. In fact, the areas of maximal coral bleaching do not correlate with where humans swim [16]! Despite this scientific evidence dispelling the postulated danger, the sale and use of sunscreens containing oxybenzone is now prohibited in Hawaii since January 2021. Two other concerns about oxybenzone are not justified. One is that oxybenzone presents estrogenic effects, demonstrated in immature rats fed extremely high doses of oxybenzone [17], comparable to doses at four times the amount usually applied to the total human body surface for 35 years [18]. Even applications of 10% oxybenzone to male and female volunteers showed no significant differences in hormone levels [19]. Although up to 1–2% systemic absorption of oxybenzone has been measured after topical application [20], the maximal concentrations noted after cutaneous absorption are too low to cause any toxicity [21]. The second concern is that oxybenzone is a contact allergen. However, only 0.07% (of 19,570 patients) [22] and 0.9% (of 23,908 patients) [23] had patch‐test positive allergies to oxybenzone. Thus, all potential concerns are not scientifically clinically valid. Inclusion of oxybenzone and other chemical sunscreen ingredients is necessary to attain the high SPF formulations which are more cosmetically appealing [23] and more effective in protecting the skin against photoaging and cancer [10]. The ability of a sunscreen to prevent UVB‐mediated erythema is measured by the internationally accepted standard sun protection factor (SPF), the ratio of equivalent exposure by UVB in sunscreen‐protected compared with unprotected skin. (An SPF of 30 means that the amount of UVB exposure in 10 minutes without sunscreen is equivalent to 10 minutes × 30 = 5 hours of exposure with sunscreen.) The SPF should be at least 30. Sunscreen labels may specify degree of UVB protection by stating that the SPF is 30+ or 50+; higher SPFs may no longer be stated on the label. SPFs higher than 30 or 50 do not double or more than triple the protection of SPF 15 when adequate amounts are applied: SPFs of 15, 30, 50, and 100 block 93%, 97%, 98%, and 99% of UVB radiation, respectively. When SPF was first defined by the FDA in 1978, the degree of protection was measured in a laboratory with application of 2 mg/cm2 of skin surface – far more than reasonably possible, requiring 4 “golf ball” or “shot glass” volumes or about 6 oz (1½–4 oz bottles) each 90 minutes when in a bathing suit. Even with generous application, most individuals apply only about ¼ that amount, yielding an effective protection of only SPF = 2.3 to a sunscreen labelled SPF 30 [24]. Therefore, applying as much as possible (at least a teaspoon to the face and to each hand and forearm) of a high SPF = 30 or 50 is recommended. Sunscreen sprays are not to be applied like quick whiffs of fragrance! Sunscreen must be sprayed generously for a full 5 seconds to each exposed site. Since some sunscreen ingredients or specific formulations may not be stable in extreme heat, do store sunscreen in the shade or within a bag under towels or, better yet, within a cooler so that application refreshes. UVA protection is measured by degree of either immediate pigment darkening (dependent upon radiation‐induced darkening of preformed melanin) or persistent (delayed) pigment darkening (as in a more complex response which induces production and transfer of melanin as well as proliferation of melanocytes). The latter assay is preferred in Europe and Japan. A sunscreen may be labeled “Broad Spectrum” only if the UVA critical wavelength (CW, the wavelength at which 90% of the UV above 320nm is absorbed) is 370nm. Only sunscreens of (1) SPF > 15 and (2) broad spectrum can claim to protect against skin cancer and photoaging. If the SPF is <15, then the label must state specifically that this sunscreen protects only against sunburn, but not against skin cancer or photoaging. Table 56.1 Criteria of a good sunscreen. SPF, sun protection factor. After SPF, the second important criterion for a sunscreen is that it be “highly water resistant,” meaning it is effective for about 80 minutes. (Labels read “water resistant” [40 minutes] or “high water resistant” [80 minutes]) The terms “waterproof” and “sweat proof” may no longer be written on sunscreen labels, since these are considered to be “false promises.” The criteria of a good sunscreen are summarized in Table 56.1. Many individuals prefer a different sunscreen for the face than for the body. This is particularly important for individuals with acne, since many ingredients that make a sunscreen formulation cosmetically smooth in texture or fragrant can be comedogenic). Further protection with topical antioxidants and sun protective clothing, hats, and sunglasses is recommended. Sun protective clothing is rated using UV protective factor (UPF), measured by the amount of UV radiation transmitted through the fabric. A fabric with a UPF of 40–50 transmits only 2.6% of biologically damaging radiation, in contrast with normal summer clothing that typically has a UPF of only 4–10, providing a maximum SPF of 30% but often only an SPF of about 2, if wet [25]. New products (such as SunGuard (2,2′‐(1,2‐ethenediyl)bis[5‐[[4‐(methylamino)‐6[[4‐(methylamino)catonyl]‐phenyl]amino]‐1,3,5‐triazin‐2‐yl]amino]‐, disodium salt)) have recently become available to be added when washing clothes to give a UPF of 30 that lasts 20 washes. Always remember the Australian motto: There are several ingredients which have been proven scientifically and clinically to protect and prevent extrinsic aging of the skin. These include retinoic acid, hydroxy acids, and certain topical antioxidants. Many products are advertised, but their efficacy may not have been demonstrated by rigorous placebo‐controlled, double‐blind clinical trials. HAs have been used for centuries. Cleopatra routinely applied the lactic acid of goat’s milk and Marie Antoinette washed with red wine, benefitting from tartaric acid. HAs were reintroduced to dermatology in 1974 when Van Scott and Yu [26] reported improvement of severe hyperkeratosis and icthyosis. HAs are classified by the position of the hydroxyl group attached to the acid moiety: α‐hydroxyacids (AHAs) (glycolic acid, lactic acid, mandelic, and citric acid), β‐hydroxyacids (BHAs) (tropic acid, salicylic acid [SA] – called a BHA but actually an α‐hydroxybenzoic acid), and the “new generation” polyhydroxy acids (PHAs) (gluconolactone or lactobionic acid – a naturally occurring component of skin). AHAs act rapidly (showing clinical improvement even within 2 weeks!) to smooth the surface skin by reducing epidermal corneocyte adhesion, first at the innermost level of the stratum corneum (just above the stratum granulosum) [27]. Epidermal damage of photoaging is corrected within 14–16 weeks, resulting in a thinned stratum corneum, epidermal acanthosis, and decreased melanogenesis [28]. An increase in epidermal intercellular hyaluronic acid improves surface moisturization by water retention. An elegant study demonstrated that epidermal keratolysis is followed by dermal penetration which increases synthesis of glycosaminoglycans and increases fibroblast proliferation and production of collagen and elastin [29]. A 25% increase in skin thickness was measured after 6 months’ treatment with 25% AHAs with no inflammation. SA is unique among the HAs in that it is lipophilic and is particularly attracted to sebaceous orifices, thereby exhibiting its keratolytic properties not only to smooth surface wrinkles, but also to decrease pore size and prevent acne. As an excellent keratolytic agent, SA solubilizes intercellular cement by disrupting corneocyte adhesion layer by layer, from the surface downward. SA may also be directly bacteriostatic. The PHAs have several advantages. They have larger molecules, so they penetrate the skin gradually and are therefore less irritating than AHAs or SA. PHAs are recommended for patients with sensitive skin, rosacea, or atopic dermatitis [28]. They can even be used in conjunction with retinoic acid without irritation. PHAs also give improved moisturization of the stratum corneum when compared with AHAs. PHAs have anti‐inflammatory and antioxidant activity, further enhancing repair of cutaneous photoaging [30]. (For further details, please see also Chapter 42: Clinical Uses of Hydroxyacids.) Three key factors determine HA efficacy: There is a delicate balance in attaining efficacy without irritation. For each type of HA or mixture thereof, the concentration and pH determines the strength and the clinical benefits [29]. Retinoids are the “gold standard” for reversing photoaging of the skin. Retinoic acid (tretinoin) has been used for more than 35 years for the treatment of acne. In the late 1980s, the remarkable clinical improvement of wrinkles and solar lentigos after treatment with topical tretinoin was documented [31–33]. UV exposure leads to decreased expression of retinoic acid receptors (RAR) and retinoic X receptors (RXR) (in particular, RAR‐α and RXR‐γ, the two major nuclear receptors in keratinocytes) with subsequent activation of transcription factors (AP‐1 and NF‐IF) which increase proliferation and inflammation and activate the matrix metalloproteinases (MMPs) that break down extracellular matrix proteins [34]. By binding to these receptors, topical retinoids restore expression, thereby reversing UV‐induced damage at all levels of the epidermis and dermis [35, 36]. (Please also consult Chapter 40: Topical Cosmeceutical Retinoids for more details about precise molecular mechanisms.) Retinoids increase epidermal proliferation causing epidermal thickening with compaction of the stratum corneum and deposition of glycosaminoglycans intercellularly; with epidermal proliferation, inhibition of excess melanogenesis and shedding of melanin‐laden keratinocytes resolves mottled hyperpigmentation; and retinoids directly induce collagen synthesis and reduce collagen breakdown by inhibiting the UV‐induced MMPs [36, 37], thereby correcting wrinkles. Topical tretinoin also reverses intrinsic aging, perhaps even more significantly in non‐sun‐exposed than in photoaged skin. A marked increase in epidermal thickness (with a more undulating dermoepidermal junction), in anchoring fibrils, and in dermal angiogenesis with new elastic fibers and glycosaminoglycans was observed [38]. Previously, topical tretinoin was postulated to make the skin more sensitive to UV exposure. Indeed, resolution of unattractive epidermal hyperkeratosis may allow more UV to penetrate deeper, but the inhibition of the UV‐induced dermal MMPs that break down collagen and elastic fibers results in less UV damage with tretinoin treatment. Occasionally, irritation (retinoid dermatitis) can occur, especially when beginning treatment. This can usually be avoided by starting with lower concentrations (0.025% cream instead of 0.05% cream or 0.01% gel) and/or less frequent application, trying other formulations (microsphere gels or new generic formulations, or using different retinoids as described below), though indeed, in the author’s opinion, tretinoin is the most effective. Patients with sensitive skin should begin with a mild formulation, applying initially every 3 days and increasing to daily over several weeks or months. Optimal improvement occurs within 6–12 months; improvement is maintained and even enhanced with continued use, as proven by up to 4‐year histologic studies [37]. Other “second generation” retinoids have been proven effective in treating photodamage [37]
CHAPTER 56
Antiaging Regimens
Introduction
Cleansing
Exfoliation
Protection
1. High SPF (SPF 30+ or preferably 50+)
2. Broad spectrum: protection against UVA and UVB
3. Highly water resistant (withstands 80 minutes of swimming)
4. Non‐comedogenic
5. Personally pleasing; lotion, gel or spray
Treatment
Hydroxyacids
Retinoids
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


