Procedure 53 Metacarpophalangeal and Proximal Interphalangeal Joint Collateral Ligament Avulsion Fractures
 See Video 39: Metacarpal Shaft Fractures
See Video 39: Metacarpal Shaft Fractures
Indications





Examination/Imaging
Clinical Examination
 Unilateral swelling and bruising of the injured joint
Unilateral swelling and bruising of the injured joint
 Lateral deviation deformity of digit due to loss of collateral ligament integrity (Fig. 53-1)
Lateral deviation deformity of digit due to loss of collateral ligament integrity (Fig. 53-1)
 Pain with restricted range of motion
Pain with restricted range of motion
 Gentle testing of collateral ligaments to ensure integrity, which may require local anesthetic block. Avoid excessive force to prevent displacement of fragment (Fig. 53-2)
Gentle testing of collateral ligaments to ensure integrity, which may require local anesthetic block. Avoid excessive force to prevent displacement of fragment (Fig. 53-2)



Imaging
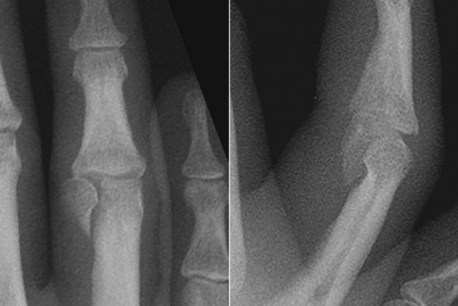
 Posteroanterior, oblique, and true lateral films of the digit for proximal interphalangeal (PIP) joint injuries. At the PIP joint, the most common avulsion fracture is a unicondylar fracture (Fig. 53-3).
Posteroanterior, oblique, and true lateral films of the digit for proximal interphalangeal (PIP) joint injuries. At the PIP joint, the most common avulsion fracture is a unicondylar fracture (Fig. 53-3).
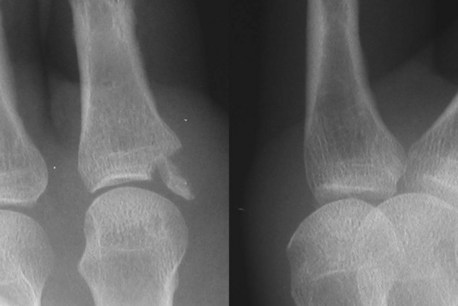
 Posteroanterior, oblique, and true lateral films of the hand for metacarpophalangeal (MCP) joint injuries (Fig. 53-4).
Posteroanterior, oblique, and true lateral films of the hand for metacarpophalangeal (MCP) joint injuries (Fig. 53-4).
 In the immature skeleton, ligament avulsion injuries occur at the growth plate with a fragment of the epiphysis (Fig. 53-5).
In the immature skeleton, ligament avulsion injuries occur at the growth plate with a fragment of the epiphysis (Fig. 53-5).



Surgical Anatomy






Exposures
Metacarpophalangeal Joint
 The MCP joint of the thumb and borders of the hand (ulnar side of small and radial side of index finger) can be easily accessed through a lateral approach.
The MCP joint of the thumb and borders of the hand (ulnar side of small and radial side of index finger) can be easily accessed through a lateral approach.
 Cutaneous nerves are located in the subcutaneous plane and must be identified and preserved.
Cutaneous nerves are located in the subcutaneous plane and must be identified and preserved.



 A Bruner zigzag skin incision is made centered over the proximal digital crease (Fig. 53-6).
A Bruner zigzag skin incision is made centered over the proximal digital crease (Fig. 53-6).
 The flexor sheath is kept intact (Fig. 53-7
The flexor sheath is kept intact (Fig. 53-7
Related posts:
 28: Pronator Teres Rerouting
28: Pronator Teres Rerouting
 33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
33: Correction of Swan-Neck Deformity in the Rheumatoid Hand
 89: Total Wrist Fusion
89: Total Wrist Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


