Fig. 1
A clinical photo (a) shows increased hindfoot valgus on the right. Weight-bearing radiographs demonstrate advanced post-traumatic osteoarthritis of the tibio-talar joint. AP (b), mortise (c), lateral (d) are seen. CT scan offers higher detail of the loss of articular cartilage, subchondral cyst formation, and subchondral sclerosis. Coronal (e) and sagittal CT (f) images are seen
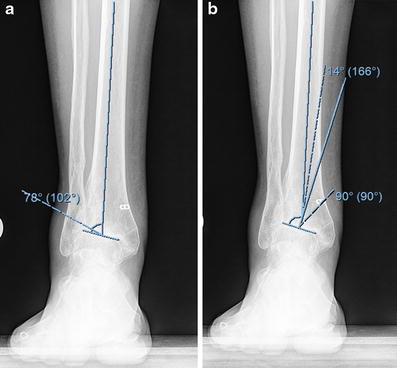
Fig. 2
(a) The lateral distal tibial angle measures 78° (normal is 90°). (b) Pre-operative planning shows a very distal CORA with a 14° valgus deformity
3 Preoperative Problem List
1.
Post-traumatic tibio-talar osteoarthritis
2.
Valgus deformity of the distal tibia
3.
Functional range of motion and young age making fusion undesirable
4 Treatment Strategy
Combined ankle distraction arthroplasty and supramalleolar osteotomy were planned. The osteotomy was stabilized with circular external fixation. A Taylor Spatial Frame (Smith & Nephew, Memphis, TN) was selected for its ability to correct deformity with great accuracy in a gradual fashion. An open arthrotomy and microfracture of the talus was also performed with injection of autologous iliac crest, bone marrow aspirate concentrate. Hinges were used to provide articulated distraction. The joint distraction was applied acutely in the operating room to 5 mm. The osteotomy of the fibula and tibia was gradually angulated to allow for an accurate bony realignment utilizing distraction osteogenesis. The foot ring would be left in place for 3 months and then removed. The tibial rings would be removed at 4 months when the osteotomy was fully healed.
5 Basic Principles
Articulated distraction: A hinge is used to preserve ankle range of motion during the 3-month treatment period.
Distraction osteogenesis: The gradual movement of an osteotomy results in bone formation at the osteotomy site. This principle was used to provide an angular correction. The valgus deformity could have been corrected acutely with a plate but would have required bone grafting or limb shortening. The accuracy of acute correction with internal fixation is less reliable than with adjustable external fixation.
6 Images During Treatment
See Fig. 3.
Get Clinical Tree app for offline access
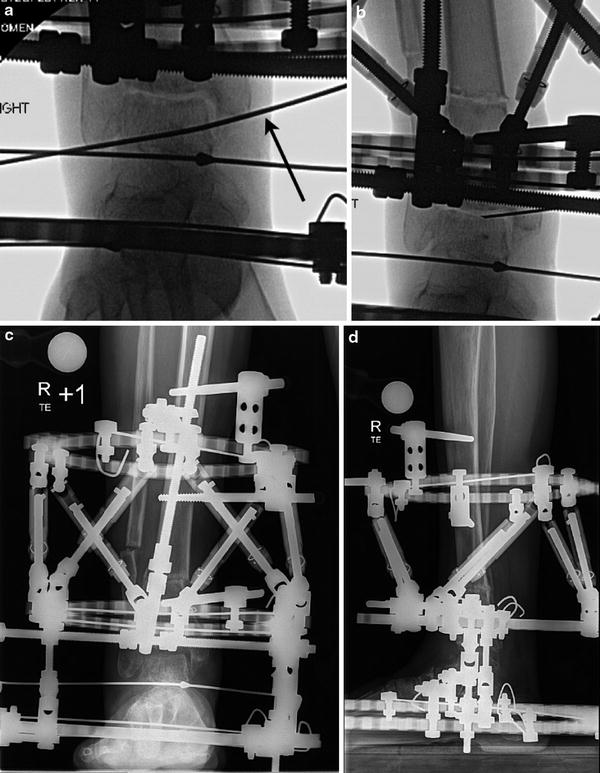
Fig. 3
The axis of ankle motion was established with an intra-articular wire (arrow) along the line created by the tips of the malleoli. (a) At the termination of the procedure, the ankle was distracted acutely, and BMAC was injected into the joint under fluoroscopy. (b
 8: Femoral Bone Defect
8: Femoral Bone Defect
 28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
 30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
28: Proximal Tibial Bone Defect Treated with Intentional Deformity and Bone Transport
30: C3.3 Pilon Fracture Closed. Ilizarov Fixation with Limited Open Reduction of Joint Surface and Distal Tibia Bridging Distraction of Ankle Joint
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
