Procedure 51 Volar Plate Arthroplasty for Dorsal Fracture-Dislocations of the Proximal Interphalangeal Joint
Indications



Examination/Imaging
Clinical Examination


Imaging
 Films of the digit, including a true lateral radiograph of the affected digit centered on the PIP joint, are required. Persistent subluxation can be recognized when the articular surface of the middle phalanx projects dorsal to a line drawn along the dorsal cortex of the proximal phalanx. Additionally, the joint space should be symmetrical both volarly and dorsally (Fig. 51-1).
Films of the digit, including a true lateral radiograph of the affected digit centered on the PIP joint, are required. Persistent subluxation can be recognized when the articular surface of the middle phalanx projects dorsal to a line drawn along the dorsal cortex of the proximal phalanx. Additionally, the joint space should be symmetrical both volarly and dorsally (Fig. 51-1).

Surgical Anatomy
 The PIP is a hinge joint with a 100- to 110-degree arc of motion. Its stability is derived from both the bony architecture of the joint and the surrounding ligamentous structures.
The PIP is a hinge joint with a 100- to 110-degree arc of motion. Its stability is derived from both the bony architecture of the joint and the surrounding ligamentous structures.


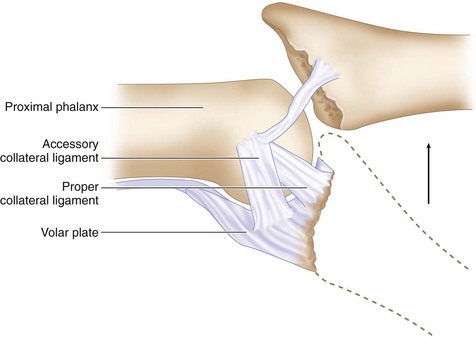
 Because the collateral ligament–volar plate complex inserts on the volar third of the middle phalanx, fractures that involve more than 30% to 40% of the volar articular segment are inherently unstable after reduction. This happens because these ligamentous restraints are attached to the fracture fragment and not to the remaining middle phalanx, which then tends to sublux dorsally. Additionally, a fracture fragment of this size also compromises the inherent bony stability by detaching the volar buttress of the articular surface that cups the proximal phalangeal condyles (Fig. 51-2).
Because the collateral ligament–volar plate complex inserts on the volar third of the middle phalanx, fractures that involve more than 30% to 40% of the volar articular segment are inherently unstable after reduction. This happens because these ligamentous restraints are attached to the fracture fragment and not to the remaining middle phalanx, which then tends to sublux dorsally. Additionally, a fracture fragment of this size also compromises the inherent bony stability by detaching the volar buttress of the articular surface that cups the proximal phalangeal condyles (Fig. 51-2).

Exposures
 A standard Bruner incision centered at the PIP flexion crease is used to expose the joint (Fig. 51-3).
A standard Bruner incision centered at the PIP flexion crease is used to expose the joint (Fig. 51-3).
 Dissection is carried down bluntly, and the radial and ulnar neurovascular bundles are identified and mobilized (Fig. 51-4).
Dissection is carried down bluntly, and the radial and ulnar neurovascular bundles are identified and mobilized (Fig. 51-4).

Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


