Procedure 49 Open Reduction and Internal Fixation of Phalangeal Shaft Spiral or Long Oblique Fractures
Indications



Examination/Imaging
Clinical Examination
 Deformity in the form of shortening, rotation, and angulation of the finger (Fig. 49-1)
Deformity in the form of shortening, rotation, and angulation of the finger (Fig. 49-1)
 Limited range of motion of the affected joint, especially the joint distal to the fracture
Limited range of motion of the affected joint, especially the joint distal to the fracture




Surgical Anatomy
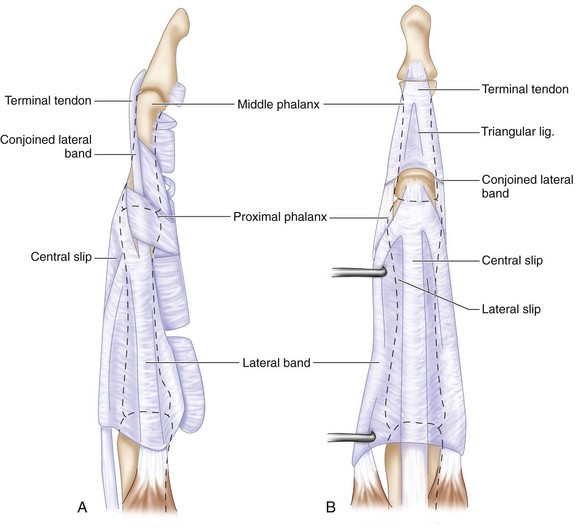
 The extensor tendons, consisting of both the extrinsic and intrinsic tendons, form a finely balanced complex over the finger (Fig. 49-3A).
The extensor tendons, consisting of both the extrinsic and intrinsic tendons, form a finely balanced complex over the finger (Fig. 49-3A).

 The fibrous flexor sheath with its flexor tendons is closely applied to the volar surface of the phalanges (Fig. 49-3B). Hence, all screws must not protrude beyond the cortex, especially on the volar aspect, to avoid attrition of the flexor tendons.
The fibrous flexor sheath with its flexor tendons is closely applied to the volar surface of the phalanges (Fig. 49-3B). Hence, all screws must not protrude beyond the cortex, especially on the volar aspect, to avoid attrition of the flexor tendons.