Fig. 1
Pre-operative radiographs prior to TTC fusion
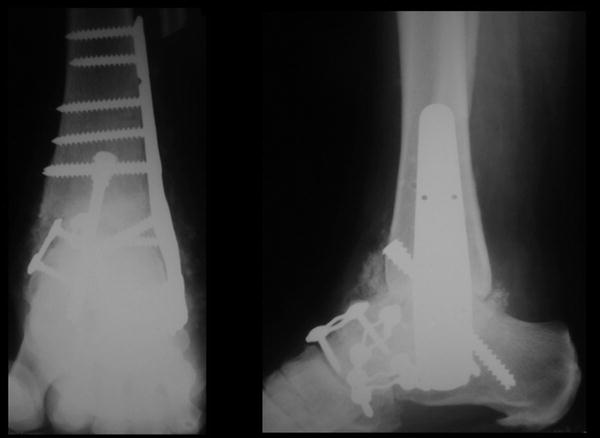
Fig. 2
Post-op after original TTC fusion lateral plate and screws
3 Preoperative Problem List
Active multi-organism infection involving a relatively fresh arthrodesis site in a diabetic patient.
Absent talus. The talus had been debrided by the original surgeon.
Open wound with a wound vac in place.
4 Treatment Strategy
The treatment strategy was to ensure that an adequate debridement of all devitalized tissue had been performed. In addition, local delivery of antibiotics via an antibiotic cement spacer is helpful in such a grossly infected situation. An antibiotic spacer is preferred to maintain the space that the talus occupied. By maintaining this space, secondary debridement in preparation for fusion and bone graft are made less complicated by preventing extensive scar tissue formation at the fusion site. One could use absorbable beads impregnated with antibiotics, then compress through this material. However, in this case it was felt that autograft would give the patient the best chance to heal.
The antibiotic spacer was to remain for at least 6 weeks or until inflammatory markers normalized. The hindfoot and ankle were grossly unstable; therefore a spanning external fixator was placed and her wounds were closed. The Taylor Spatial Frame was chosen because it could act as a static frame initially, then at the second stage of treatment, it could provide gradual docking and compression of the tibia to the calcaneus.
The antibiotic spacer remained for 8 weeks. The patient’s infection had been eradicated and a staged procedure was performed to remove the antibiotic spacer and place iliac crest bone graft between the tibia and calcaneus. Iliac crest bone graft is the “gold standard” and in challenging cases gives the patient the best chance to heal bone. Other options are available, including no bone grafting, but are less desirable in salvage situations. The Taylor Spatial Frame was then used to gradually close the space between the tibia and calcaneus and ultimately compress these bones for arthrodesis.
5 Basic Principles
Basic principles included eradication of infection with wide debridement of devitalized tissue, stable external fixation, and local and intravenous delivery of culture-specific antibiotics. Once the infection is eradicated, a staged spacer removal and arthrodesis of the tibia to the calcaneous can be performed. Gradual docking of the tibia to the calcaneus was utilized because an acute correction would have caused the soft tissue to compress and form a “donut,” resulting in tension on the wound closure and compression of vascular supply to the foot. One can typically acutely shorten up to 3 cm. Beyond this distance, a gradual shortening allows the tissue to accommodate this compression.
Once the fusion site is compressed, one can perform a recompression using the spatial frame software at regular intervals during the patient’s care. There are different opinions as to the timing of these compressions. In this case, it was performed at the 3-week post-op visit and the 6-week post-op visit.
6 Images During Treatment
See Figs. 3, 4, 5, 6, and 7.
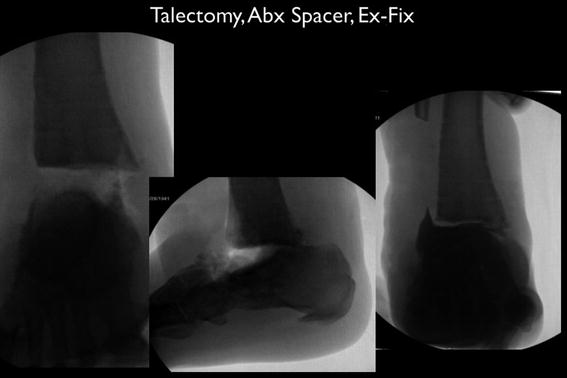
Fig. 3
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 78: Two-Stage Treatment of a Chronic Foot Dislocation
78: Two-Stage Treatment of a Chronic Foot Dislocation
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
78: Two-Stage Treatment of a Chronic Foot Dislocation
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
