Procedure 48 Open Reduction and Internal Fixation of Phalangeal Unicondylar Fractures
 See Video 38: ORIF of Middle Phalanx Volar Avulsion Fracture
See Video 38: ORIF of Middle Phalanx Volar Avulsion Fracture
Indications
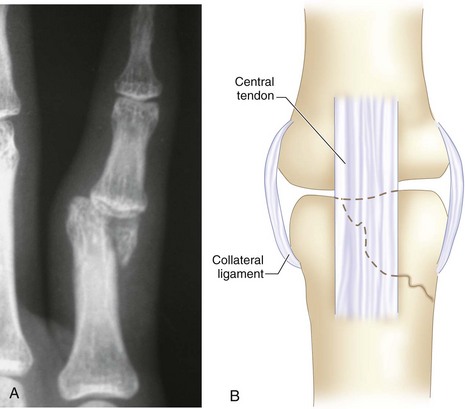
 Fractures of phalangeal condyles are classified by Weiss and Hastings into various subtypes. The most common is the displaced unicondylar fracture. The obliquity of the fracture line makes it highly unstable and liable to displacement. Nonoperative treatment is often unsuccessful in maintaining the reduction of the fracture. The condylar fragment also bears the origin of the important collateral ligament. The displacement of the fractured condyle therefore results in disruption of articular congruity, joint instability, angular deformity, and loss of joint motion. A displaced condylar fracture is an indication for open reduction and internal fixation.
Fractures of phalangeal condyles are classified by Weiss and Hastings into various subtypes. The most common is the displaced unicondylar fracture. The obliquity of the fracture line makes it highly unstable and liable to displacement. Nonoperative treatment is often unsuccessful in maintaining the reduction of the fracture. The condylar fragment also bears the origin of the important collateral ligament. The displacement of the fractured condyle therefore results in disruption of articular congruity, joint instability, angular deformity, and loss of joint motion. A displaced condylar fracture is an indication for open reduction and internal fixation.






Surgical Anatomy
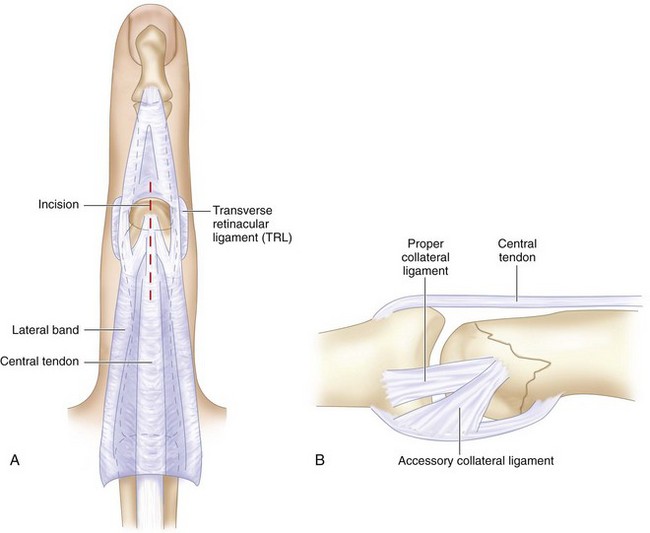
 Midline central tendon splitting approach gives good exposure of the proximal interphalangeal joint. Flexion of the joint and retraction on the tendon allow the extensor tendon to slip around both condyles, giving excellent visualization of nearly the whole dorsal and distal extent of the condyles (Fig. 48-2A).
Midline central tendon splitting approach gives good exposure of the proximal interphalangeal joint. Flexion of the joint and retraction on the tendon allow the extensor tendon to slip around both condyles, giving excellent visualization of nearly the whole dorsal and distal extent of the condyles (Fig. 48-2A).
 To avoid avascular necrosis, blood supply to the fractured condyle should be carefully preserved. The fractured condyle should not be detached from the palmar soft tissue attachment and collateral ligament (Fig. 48-2B).
To avoid avascular necrosis, blood supply to the fractured condyle should be carefully preserved. The fractured condyle should not be detached from the palmar soft tissue attachment and collateral ligament (Fig. 48-2B).