Procedure 43 Carpal Wedge Osteotomy for Congenital Wrist Flexion Contracture (Arthrogryposis)
 See Video 35: Triceps Lengthening and Elbow Release in Arthrogryposis
See Video 35: Triceps Lengthening and Elbow Release in Arthrogryposis



Examination/Imaging
Clinical Examination
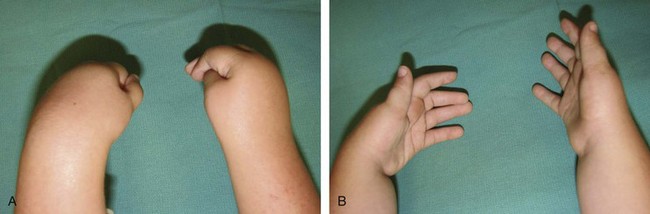
 The ability of the child to open and close the fingers should be determined. If the child does not have active finger extension, correction of the wrist flexion contracture will result in loss of ability to passively extend the finger by the tenodesis effect (Fig. 43-3).
The ability of the child to open and close the fingers should be determined. If the child does not have active finger extension, correction of the wrist flexion contracture will result in loss of ability to passively extend the finger by the tenodesis effect (Fig. 43-3).





Positioning


Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


