Procedure 41 Centralization for Radial Longitudinal Deficiency
 See Video 34: Centralization for Radial Deficiency
See Video 34: Centralization for Radial Deficiency
Indications
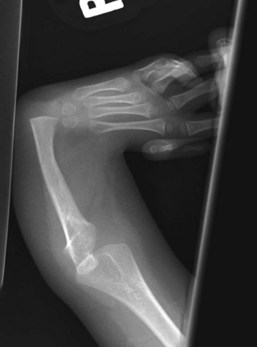
 Radial longitudinal deficiency (RLD) has been classified into four grades depending on the degree of hypoplasia of the radius (Table 41-1). Centralization is usually performed at 9 to 12 months of age because anesthesia is safer, preliminary soft tissue distraction can be carried out, and subsequent thumb reconstruction can be done before the child develops a maladaptive pattern.
Radial longitudinal deficiency (RLD) has been classified into four grades depending on the degree of hypoplasia of the radius (Table 41-1). Centralization is usually performed at 9 to 12 months of age because anesthesia is safer, preliminary soft tissue distraction can be carried out, and subsequent thumb reconstruction can be done before the child develops a maladaptive pattern.
 This procedure may be done first for children with type 0 or 1 deficiencies.
This procedure may be done first for children with type 0 or 1 deficiencies.

Table 41-1 Classification of Radial Longitudinal Deficiency
| Type | Distal Radius | Proximal Radius |
|---|---|---|
| N | Normal | Normal |
| 0 | Normal | Normal, radioulnar synostosis, congenital radial head dislocation |
| 1 | >2 mm shorter than ulna | Normal, radioulnar synostosis, congenital radial head dislocation |
| 2 | Hypoplasia | Hypoplasia |
| 3 | Physis absent | Variable hypoplasia |
| 4 | Absent | Absent |
Examination/Imaging
Clinical Examination
 Sixty percent to 70% of children with RLD have an associated systemic or musculoskeletal abnormality, the most common being scoliosis. Therefore, before surgery, all children with RLD should undergo a thorough musculoskeletal and systemic examination, including spinal radiographs, cardiac echocardiographic evaluation, renal ultrasound, and a complete blood count.
Sixty percent to 70% of children with RLD have an associated systemic or musculoskeletal abnormality, the most common being scoliosis. Therefore, before surgery, all children with RLD should undergo a thorough musculoskeletal and systemic examination, including spinal radiographs, cardiac echocardiographic evaluation, renal ultrasound, and a complete blood count.